Running Head: Peak Inspiratory Flow Rate in COPD
Funding Support: Funding for this project was provided by Sunovion Pharmaceuticals, Inc.
Date of Acceptance: April 21, 2017
Abbreviations: peak inspiratory flow rate, PIFR; chronic obstructive pulmonary disease, COPD; dry powder inhaler, DPI; metered dose inhalers, MDI; soft mist inhalers, SMI; modified Medical Research Council, mMRC; COPD Assessment Test, CAT; Morisky Medication Adherence Scale, MMAS; forced expiratory volume in 1 second, FEV1; forced vital capacity, FVC; body mass index, BMI; length of stay, LOS; short-acting beta-agonist, SABA; short-acting muscarinic antagonist, SAMA; long-acting muscarinic antagonist, LAMA; long-acting beta2-agonist, LABA; inhaled corticosteroids, ICS
Citation: Sharma G, Mahler DA, Mayorga VM, Deering KL, Harshaw Q, Ganapathy V. Prevalence of low peak inspiratory flow rate at discharge in patients hospitalized for COPD exacerbation.
Chronic Obstr Pulm Dis. 2017; 4(3): 217-224. doi:
http://doi.org/10.15326/jcopdf.4.3.2017.0183
Introduction
Chronic lower respiratory disease, primarily chronic obstructive pulmonary disease (COPD), was the third leading cause of death in the United States in 2013, claiming the lives of 149,205 Americans.1 COPD treatment involves the use of both short- and long-acting beta2-agonists and, more recently, muscarinic antagonists that are delivered through devices such as metered-dose inhalers (MDIs), dry powder inhalers (DPIs), soft mist inhalers (SMIs), and nebulizers.2 Each type of device has its own advantages and disadvantages in terms of delivery effectiveness versus motor coordination techniques. MDIs require complex coordination techniques with a slow inhalation by the patient to achieve a clinically effective dose.3,4 DPIs decrease the complexity of administration, but effective medication delivery is dependent on the force of the patient’s inspiratory effort to overcome internal resistance.5 A relatively recent addition to the COPD market, SMIs deliver medication in a slow-moving mist independent of the patient’s inspiratory effort and are less dependent on inhalation technique.6 Nebulizers are machines that deliver medication in a way that is independent of inspiratory effort and inhalation technique.7
DPIs have internal resistance and some patients may not be able to inhale an optimal amount of powder deep into the lower respiratory tract. Peak inspiratory flow rate (PIFR), the measure of a patient’s inspiratory effort, can be used to assess a patient’s ability to generate adequate inspiratory flow rate from DPIs such as the DISKUS®. The literature suggests that a PIFR below 60 L/min in COPD patients may result in ineffective inhalation of medications.8-10 We hypothesize that ineffective inhalation of medications due to low PIFR can result in poor COPD management and adverse consequences for the patient. Given that COPD generally affects an older, multi-morbid population, the mode of medication delivery may, therefore, be an important consideration for clinicians when selecting a treatment, especially upon discharge for a COPD exacerbation.
The prevalence of low PIFR in patients being discharged for a COPD exacerbation has not been studied to date. Generally, discharge protocols for COPD patients do not include an assessment of PIFR or patients’ ability to use their inhaler device when they recuperate after discharge. The objectives of this analysis were to evaluate the prevalence of and factors associated with low PIFR, the real-world treatment patterns by PIFR levels, and rehospitalizations among COPD patients at discharge from the hospital following an exacerbation.
Methods
This was an institutional review board–approved prospective, observational study of patients hospitalized for a COPD exacerbation at 7 sites in the United States. Patients were identified and screened for enrollment if they had a primary or secondary COPD diagnosis for the admission in their medical records and had a diagnosis of COPD for at least 1 year. All screened patients provided a PIFR value, which was measured using the InCheckTM DIAL, a device that has been widely used in previous studies.8,11-15 According to the manufacturer, the InCheckTM DIAL is accurate to +/− 10% or 10 L/min, whichever is greater, and can measure flows in the range of 15 to 120 L/min.16 The InCheckTM DIAL was set to simulate resistance of the DISKUS® DPI, a commonly used DPI device and has a lower resistance than the Handihaler® and Turbuhaler®.12,17 Patients made 3 PIFR attempts, and study coordinators instructed each patient to inhale as quickly as possible with the InCheckTM DIAL after a complete exhalation.
The highest PIFR value for each enrolled patient was recorded and used for analysis and classification8,11,12,13 into the low PIFR (<60 L/min) or normal PIFR (≥60 L/min) cohorts. A cutoff of 60 L/min was selected between the low and normal cohorts because the literature suggests that the optimal PIFR against the internal resistance of a DPI is at least 60 L/min.8-10 To maintain the observational nature of the study, PIFR measurement was not shared with the treating provider. Patients were recruited for enrollment between May 19, 2015 and March 1, 2016. Cohort enrollment was actively managed to achieve equal numbers of patients in the low and normal PIFR cohorts.
Demographics, clinical characteristics, COPD-related health status, and treatment data were collected for the patients who were enrolled in the study. The level of activity limitation or disability due to dyspnea was assessed with the modified Medical Research Council (mMRC) dyspnea scale, and the COPD-related health status and symptom burden was assessed with the COPD Assessment Test (CAT) score for the patients who were enrolled in the study. The mMRC dyspnea scale and the CAT score were selected because they are recommended in the Global initiative for chronic Obstructive Lung Disease (GOLD) strategies to define COPD symptom burden.2 The Morisky Medication Adherence Scale (MMAS), a widely used self-reported measure of adherence, was also collected for the enrolled patients. Scores on the MMAS range from 0 to 4, with a score of zero reflecting high adherence, scores of 1 and 2 reflecting medium adherence, and scores of 3 and 4 reflecting low adherence. All baseline data, including PIFR, were collected by study coordinators within the 24 hours prior to the discharge date.
Rehospitalization data to the index hospital system were collected via chart review for the 30, 31-90 and 180 days following index hospitalization.
Descriptive analysis was performed according to the study objectives. Prevalence of low PIFR (<60 L/min) was calculated using data from all patients screened for enrollment. Differences between low and normal PIFR cohorts were tested using chi-squared tests for proportions and Student’s t-tests for continuous measures. McNemar’s test was used to examine the change in patients’ medication use between admission and discharge. Multiple logistic regression models were used to examine the predictors of low PIFR in the total patient population and in the subgroup of patients with pulmonary function tests. A p value of ≤ 0.05 was considered statistically significant. All analyses were performed using SAS version 9.2 (SAS Institute, Cary, North Carolina).
Results
A total of 268 patients were screened for enrollment. To achieve equal cohorts, 98 patients with normal PIFR (≥60 L/min) were excluded from further analysis after PIFR data were collected. A total of 170 patients were enrolled, with 85 patients enrolled in both the low and normal PIFR cohorts.
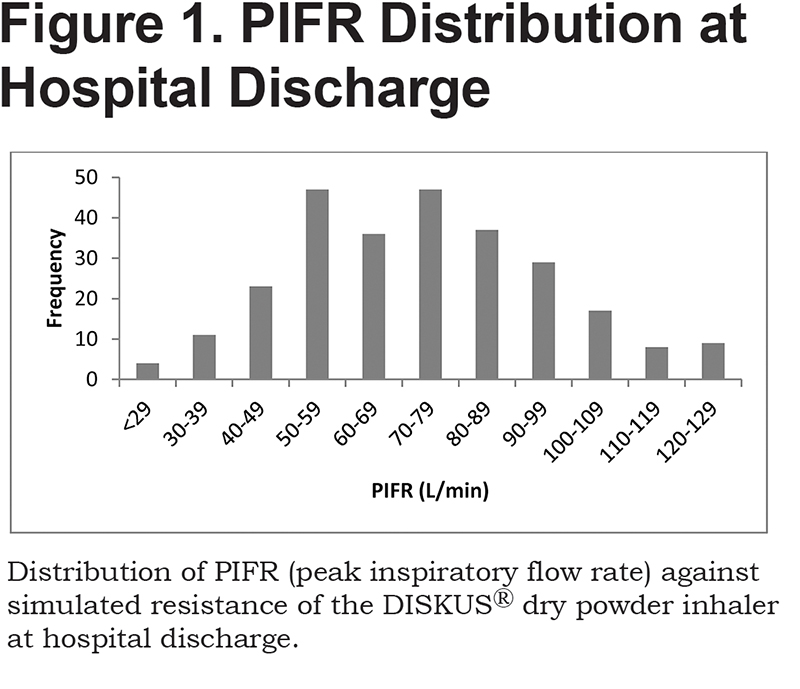
The mean PIFR for the 268 patients screened for enrollment was 71 ± 22.12 L/min. Low PIFR (<60/min) was observed in 31.7% (85/268) of patients (Figure 1). Of the 85 patients with low PIFR, 15 (18%) had a PIFR less than 40 L/min, 23 patients (27%) had a PIFR between 40-49 L/min, and 47 (55%) had a PIFR between 50-59 L/min.
Demographic characteristics, clinical characteristics, and COPD-related health status data for the enrolled patients (n = 170) is presented in Table 1. Among all enrolled patients, those in the low PIFR cohort were older (66.2 ± 10.04 years versus 62.1 ± 9.41 years, p = 0.006) and were more likely to be women (61.2% versus 42.4%, p = 0.014) compared with patients with normal PIFR. Mean height was similar between patients in the low and normal PIFR cohorts (65.6 ± 3.85 versus 66.4 ± 3.99 inches, p = 0.193) and there was no difference in the height of women between the low and normal PIFR cohorts (63.7 ± 3.00 versus 64.2 ± 4.01 inches, p = 0.496). Based on the most recent pulmonary function tests, the mean forced expiratory volume in 1 second (FEV1) percent predicted was between 30% and 49% of the normal range, suggesting severe disease.
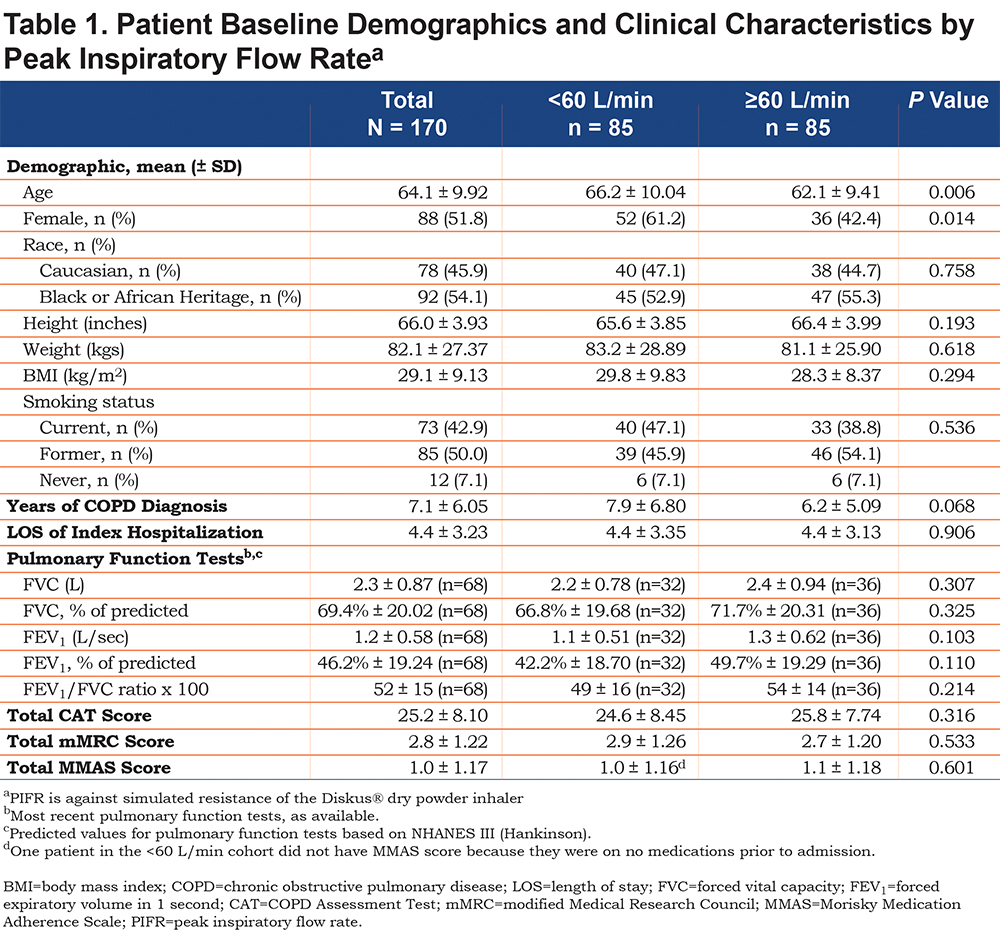
There was no statistically significant difference in mMRC dyspnea score or CAT score between the low and normal PIFR cohorts. The mean CAT scores of patients were above 20, suggesting a high impact of COPD on the patients’ health status, regardless of the PIFR (Table 1). Over 90% of patients in both the low and normal PIFR cohorts had a total CAT score ≥10, the cutoff for higher symptom burden in the GOLD strategies.2 The mean mMRC dyspnea scores indicated that patients were symptomatic with daily activities in both PIFR cohorts. Over 80% of patients in both the low and normal PIFR cohorts had a total mMRC dyspnea score ≥2, the cutoff for higher symptom burden in the GOLD strategies.2 No statistically significant correlation was found between PIFR and CAT score (p = 0.536) and PIFR and mMRC dyspnea score (p = 0.148). The mean MMAS score indicated medium medication adherence in both PIFR cohorts, and there was no difference between the cohorts. Multiple logistic regression analysis was performed to predict low PIFR with patient demographics and disease severity measures as predictors. Compared to men, women showed a greater chance of having low PIFR (odds ratio = 2.411, p= 0.0457). As age increased, the chance to have low PIFR also increased (odds ratio = 1.052, p = 0.0058). Compared to nonsmokers, the chance to have low PIFR was twofold higher for current smokers (odds ratio = 2.055, p= 0.0422).
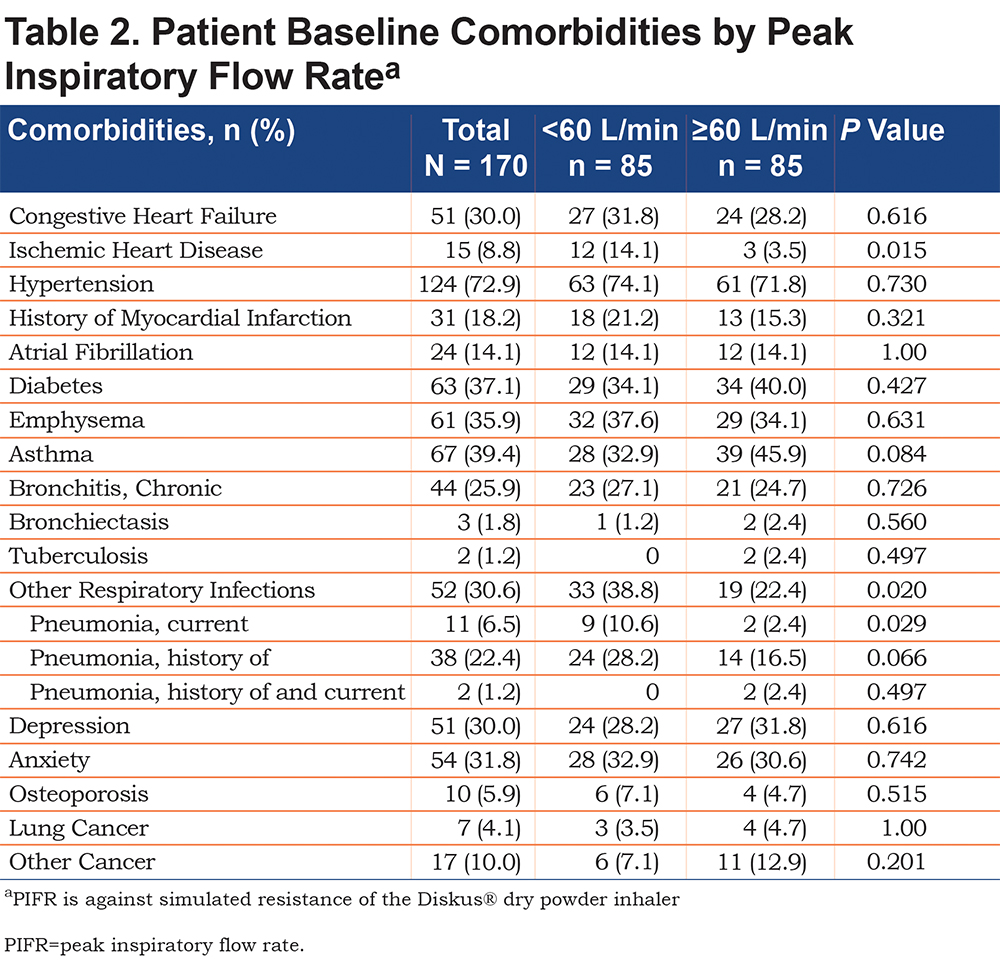
In the analysis of comorbidities at enrollment (Table 2), pneumonia was a more common comorbidity among patients in the low PIFR cohort (38.8% versus 22.4%, p = 0.020). There were more patients in the low PIFR cohort with a current diagnosis of pneumonia (10.6% versus 2.4%, p = 0.029) and there was a trend towards increased history of pneumonia in the low PIFR cohort (28.2% versus 16.5%, p = 0.066). Comorbid ischemic heart disease was also more common in the low PIFR cohort (14.1% versus 3.5%, p = 0.015).
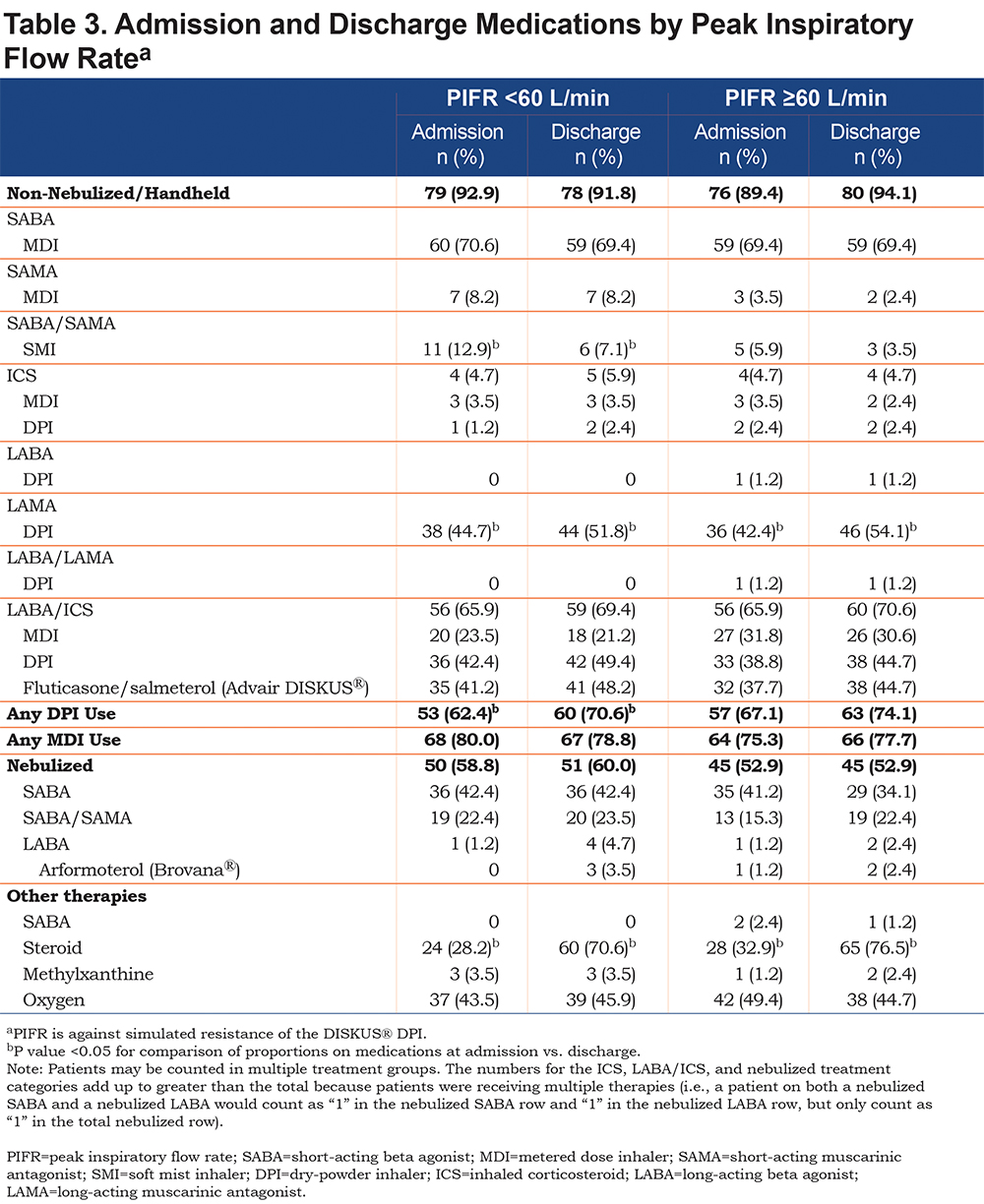
Treatments at discharge following index hospitalization were similar to those at the time of admission in both cohorts (Table 3), with a few exceptions. As expected, the use of intravenous/oral corticosteroid was higher at discharge compared with at admission in both cohorts (low PIFR: 28.2% versus 70.6%, p < 0.0001; normal PIFR: 32.9% versus 76.5%, p < 0.0001). The short-acting beta-agonist (SABA)/short-acting muscarinic antagonist (SAMA) SMI use was lower at discharge compared with at admission in the low PIFR cohort (12.9% versus 7.1%, p = 0.025). More patients were discharged on a long-acting muscarinic antagonist (LAMA) DPI in both cohorts (low PIFR: 44.7% versus 51.8%, p = 0.034; normal PIFR: 42.4% versus 54.1%, p = 0.012). There was a trend towards increased long-acting beta2-agonist (LABA)/inhaled corticosteroids (ICS) DPI use in the low PIFR cohort at discharge (42.4% versus 49.4%, p = 0.058). There was increased DPI use in the low PIFR cohort at discharge, with 62.4% of patients in the low PIFR cohort receiving bronchodilator medications via a DPI device at admission and 70.6% at discharge (p = 0.020). More than half of the patients in both the low and normal PIFR cohorts were discharged with a nebulized therapy (60.0% and 52.9%, respectively).
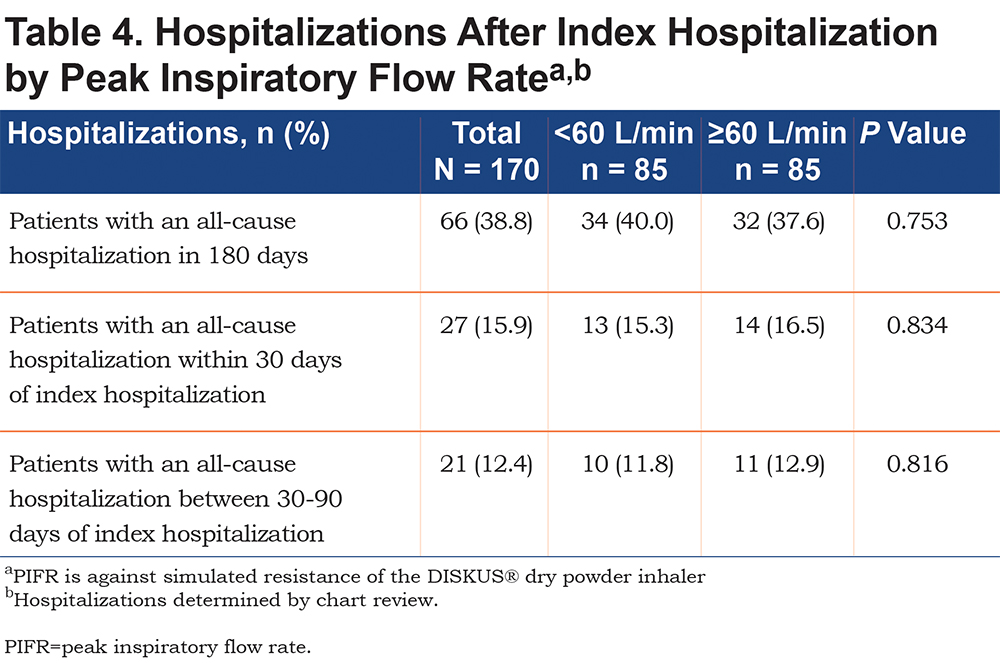
All-cause rehospitalizations were similar between the low and normal PIFR cohorts during the follow-up period (Table 4). The incidences of all-cause rehospitalization at 30, 31-90 and 180 days following index hospitalization were: 15.3%, 11.8% and 40% respectively in the low PIFR cohort and 16.5%, 12.9% and 37.6% respectively in the normal PIFR cohort (p values for differences not significant for any time point).
Discussion
The mean PIFR at discharge following hospitalization for an exacerbation of COPD was 71 ± 22.12 L/min, and 31.7% of patients had PIFR less than 60 L/min. To our knowledge, our results are the first to describe the prevalence of low PIFR in patients at discharge following hospitalization for an exacerbation of COPD. Prior studies8,12,13 have assessed PIFR in clinically stable patients with COPD. A COPD exacerbation may have a deleterious effect on peak inspiratory flow due to lung hyperinflation. Therefore, it is important to measure PIFR at discharge to determine whether the patient can adequately inhale dry powder from a DPI, if such medication is prescribed.
Our PIFR cohorts are based on the literature demonstrating a PIFR over 60 L/min is considered optimal.8,12,18 We found the prevalence of low PIFR (<60 L/min) to be 31.7% following hospitalization for a COPD exacerbation. In a study in the outpatient setting of patients with advanced COPD, Mahler and colleagues13 found the prevalence of PIFR less than 60 L/min to be 19%. Additionally, we found patients in the low PIFR cohort following hospitalization for a COPD exacerbation to be older and more likely to be women, with no differences in height or pulmonary function tests between cohorts. Mahler et al13 found that the majority of patients with PIFR less than 60 L/min were women, of shorter height, and with lower percent predicted forced vital capacity (FVC) and inspiratory capacity. The differences in enrolled patient populations and timing of PIFR measurement may account for the different study results. Study findings suggested that pneumonia and ischemic heart disease were associated with low PIFR. The clinical rationale for these findings are not clear and could be a reflection of unobserved confounders due to low sample sizes.
Our data suggest that PIFR did not impact all-cause rehospitalizations up to the 180-day follow-up period. However, it should be noted that the study was not powered for these outcomes and there was only a small sample of patients with rehospitalizations. Additionally, the analysis did not control for medication use and hospitalizations outside the index hospital system. Further, large studies are needed for evaluating impact of PIFR on rehospitalization.
PIFR can be used to assess a patient’s ability to generate adequate inspiratory flow rate, and thus can be used to guide COPD treatment choices. DPIs have internal resistance and patients with diminished PIFR may not be able to inhale medications using a DPI effectively into the lower respiratory tract. Despite the patient’s inability to generate optimal inspiratory flow, nearly two-thirds of patients in the low PIFR cohort received bronchodilator medications via a DPI device at discharge for a COPD exacerbation. Existing discharge protocols for COPD patients typically do not include an assessment of PIFR at discharge for a COPD exacerbation. Prior to our study, the number of patients discharged who are unable to generate adequate peak inspiratory flow was unclear. Our study aimed to identify the prevalence of low PIFR in this patient population and highlight the use of DPIs at discharge in patients for whom these inhalation devices may not be effective.
There are a few limitations to note in our study. First, we measured PIFR only against the simulated resistance of the DISKUS® DPI. We chose the DISKUS® DPI because it is a commonly used DPI device, and because the DISKUS® DPI has lower internal resistance than the Handihaler® and Turbuhaler® DPIs.8,10,12 Second, sites used multiple coordinators administering the PIFR reading with the InCheckTM DIAL. Site coordinators were trained on the use of the InCheckTM DIAL; however, there could be inter-observer differences in technique. Third, data recorded for tiotropium did not specify whether the inhaler used was a DPI or SMI. Upon verification with the study sites that the majority of tiotropium use was DPI, the decision was made to categorize this medication as a DPI for analysis. Fourth, the admission diagnosis was used to identify patients for this study, and may have been updated from COPD exacerbation to congestive heart failure exacerbation after discharge for a small number of patients. Due to the similarities in patient treatments, these patients were not excluded from further analysis. Finally, enrollment numbers were not consistent across study sites, and thus site-specific treatment patterns could have had an influence on our overall results.
In conclusion, approximately one-third of COPD patients had a low PIFR (<60 L/min) prior to discharge from hospitalization following an exacerbation of COPD. Patients in the low PIFR group were older and more likely to be female. Future research is needed to understand the optimal treatment of patients with low PIFR compared with patients with normal PIFR.
Acknowledgments
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript by contributing to conception, design, or data process; drafting and critically revising the manuscript; and approving this draft for submission and accepting responsibility for the contents within. Authors wish to thank Claudette Knight, PharmD, of Percolation Communications for medical editorial assistance. Financial support for medical editorial assistance was provided by Sunovion Pharmaceuticals, Inc.
Declaration of Interest
Gulshan Sharma serves on the scientific advisory board at Sunovion Pharmaceuticals, Inc. Donald A. Mahler serves on an advisory board and a speaker’s bureau for Sunovion Pharmaceuticals, Inc. Valerie M. Mayorga, Kathleen L. Deering, and Qing Harshaw are employed at EPI-Q, Inc., which received funding from Sunovion Pharmaceuticals, Inc., for this analysis. Vaidyanathan Ganapathy is a full-time employee of Sunovion Pharmaceuticals, Inc. The content of this manuscript, the ultimate interpretation, and the decision to submit for publication was made by the authors independently.