Running Head: Pharmacist Comprehensive and Collaborative Transitions of Care
Funding support: No funding was provided in direct support of this research
Date of acceptance: November 16, 2020 | Published online: November 19, 2020
Abbreviations: chronic obstructive pulmonary disease, COPD; emergency department, ED; confidence interval, CI; hazard ratio, HR; number needed to harm, NNH; Centers for Medicare and Medicaid Services, CMS; Hospital Readmissions Reduction Program, HRRP; diagnosis-related group, DRG; electronic health record, EHR; primary care provider, PCP; forced expiratory volume in 1 second, FEV1; Global initiative for chronic Obstructive Lung Disease, GOLD; long-acting muscarinic antagonist, LAMA; long-acting beta2-agonist, LABA
Citation: Kim J, Lin A, Absher R, Makhlouf T, Wells C. Comprehensive and collaborative pharmacist transitions of care service for underserved patients with chronic obstructive pulmonary disease. Chronic Obstr Pulm Dis. 2021; 8(1): 152-161. doi: http://doi.org/10.15326/jcopdf.2019.0175
Introduction
Chronic lower respiratory disease is the fourth leading cause of death in the United States.1 Risk of mortality from chronic obstructive pulmonary disease (COPD) increases significantly in the first year after readmission within 30 days of a hospitalization (hazard ratio [HR] 2.48, 95% confidence interval [CI] 1.10–5.59).2 For patients readmitted within 30 days, the estimated absolute increase in mortality risk is 4% at 30 days (number needed to harm [NNH], 25), 17% at 6 months (NNH, 6), 19% at 1 year (NNH, 6) and 24% at 3 years (NNH, 5).2 The 5-year mortality rate is 40%-70% depending on COPD severity. For patients with severe disease, the 2-year mortality rate is about 50%.3
In the past, the U.S. health care system was sustained by prospective payment, minimizing hospital length of stay and maximizing turnover.4 To improve quality of care and reduce readmissions risks, the Centers for Medicare and Medicaid Services (CMS) Hospital Readmissions Reduction Program (HRRP) became effective in 2012.5 Hospitals were penalized up to 1% of diagnosis-related group (DRG) payments (this penalty increased to 3% in 2015) for excess readmissions, totaling nearly $1.9 billion in penalties.6 In 2013, myocardial infarction, heart failure, and pneumonia were included in the HRRP 30-day readmission penalties. By 2015, CMS added COPD and elective hip or knee replacement to these conditions. The Agency of Healthcare Research and Quality also considers COPD an ambulatory care-sensitive condition for which outpatient care can reduce hospitalization.7
On average, a COPD-related emergency department (ED) visit costs $647, while an admission ranges from $7,242 (simple) to $44,909 (intensive care unit with intubation).8 These costs increase over the years, and costs can be compounded by continuous readmissions. Around 20% of patients hospitalized for COPD exacerbation are readmitted within 30 days of discharge.2 Additionally, a history of 2 or more exacerbations in the previous year predicts the 30-day readmission of COPD patients2 (HR, 2.47; 95% CI 1.51–4.05), suggesting that many opportunities exist to prevent readmissions and their associated consequences.
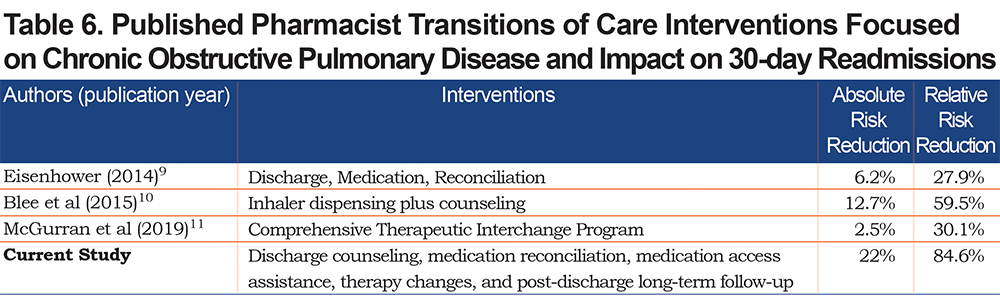
Pharmacists have been increasingly involved in reducing readmissions, with an array of activities including discharge counseling, medication reconciliation, therapy changes, dispensing, post-discharge phone calls, and face-to-face visits.9-24 The National Transitions of Care Coalition supports pharmacist inclusion to help reduce readmissions.25 Specific to COPD, pharmacist discharge medication reconciliation for elderly (N=29) reduced 30-day readmissions9 from 22.2% to 16.0%. Another study of pharmacists dispensing inhalers and providing discharge counseling (N=620) reduced 30- and 60-day readmissions from 21.4% to 8.7% (p=0.0016), and 33% to 23% (p=0.0056), respectively.10 A therapeutic interchange program for COPD patients was associated with reduced 30-day readmissions (8.3% of 1535 control patients versus 5.8% of 1350 intervention patients; P=0.012), in addition to reduced average inhaled medication costs from $311 to $221 (P < 0.01).11 The purpose of this study is to evaluate a comprehensive and collaborative pharmacist COPD transitions of care service.
Methods
Setting
The study site was a primary care internal medicine residency clinic located within a 536-bed community teaching hospital. Of approximately 2000 total patients, the payer mix consists of 45% Medicare, 17% Medicaid, 19% commercial, and 20% uninsured. The clinic serves adult patients regardless of financial or insurance status. An estimated 50%-70% of the population is underserved, approximately 69% are Black, 24% are White, 60% are female, and 40% are male.
Clinical Process
A pharmacist was added to the internal medicine residency team in 2015. At that time, attending physicians requested pharmacist involvement with transitions of care. The hospital’s 30-day readmission rate for COPD was 19.6%, which was consistent with the national average.26 For the transitions of care daily workflow (Figure 1), pharmacists identified patients using an electronic health record (EHR) function called patient lists. All patients admitted to the hospital while a pharmacist was on service, whose primary care provider (PCP) was on the internal medicine residency team, were reviewed by the pharmacist, who then provided discharge counseling, medication reconciliation, medication access assistance, and therapy optimization (contacted physicians with recommendations and implemented changes).
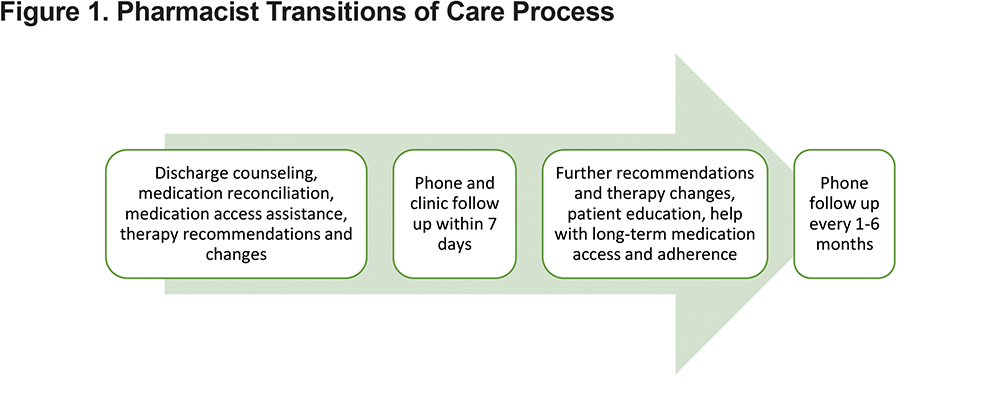
After discharge, the pharmacist called patients by phone within 1 week to further evaluate medication use and symptoms (Figure 1). At clinic appointments, a pharmacist met with patients, PCPs, and nurses to complete medication reconciliation and assist with other interventions (e.g., vaccines, smoking cessation) and education. During these visits, the pharmacist collaborated with the clinic social worker and financial counselor, as well as community pharmacies, if needed for medication access. Following clinic visits, the pharmacist called patients monthly for 3 months, and then every 3–6 months. The pharmacist utilized teach-back during all patient interactions and provided handouts during face-to-face encounters.
Other pharmacist activities included COPD education to attending and resident physicians annually (1-hour lecture, 30-minute device education). Additionally, pharmacists procured and managed inhaled medication samples (bronchodilators, inhaled corticosteroids) for immediate access, and helped with long-term medication access as well. Pharmacy residents and students on rotation participated in all activities.
Design
This is a retrospective study approved by the health system’s institutional review board. Adult patients were included if they had a PCP from a physician residency clinic and were admitted to the hospital with a primary diagnosis of COPD (diagnosis-related group codes beginning with J44.0)27 during a 3-year period (May 2016 through April 2019). Patients who received pharmacist intervention as described above were assigned to the intervention group; those who did not receive the service were assigned to the usual care group. Each new patient admission during this time period was counted as an index admission. Subsequent admissions for the same patients were only counted as additional index admissions if they occurred more than 180 days after the first index admission. Hospitalizations were excluded if they were not found in the EHR due to occurring within another health system without electronic charting or with an EHR that does not interface with the EHR used in the study, or for patients with PCPs outside the study health system.
Data Analysis
The primary outcome was a composite of COPD-related hospital admissions and ED visits. Secondary outcomes include 30-, 60-, 90-, 180-day COPD-related hospital admissions and ED visits, associated costs, pharmacist interventions, time to follow-up, and pneumonia. Hospital visits were evaluated by chart review; any requiring acute treatment for COPD were considered COPD-related. ED visits resulting in hospital admissions were counted as hospital admissions rather than individual ED visits. Associated costs described in the literature were used for the cost analysis (average COPD-related ED visit $647, simple admission $7,242, intensive care unit with intubation $44,909).8
A power calculation was performed after implementation of the pharmacist service but prior to data collection and analysis using PASS software (version 16.0.1, NCSS LLC, Kaysville, Utah).28 Stata software (version 15.2, Stata Corporation, College Station, Texas) was utilized to analyze data.29 The estimated sample size needed was 50 index admissions (power=0.80 with a 2-sided alpha of 0.05) to detect an anticipated 66% relative risk, presuming a readmission rate of approximately 35% based on internal data. Visit data, length of stay, and costs were compared using t-tests (paired t-tests for pre-post data). Pharmacist interventions were characterized with descriptive statistics.
Results
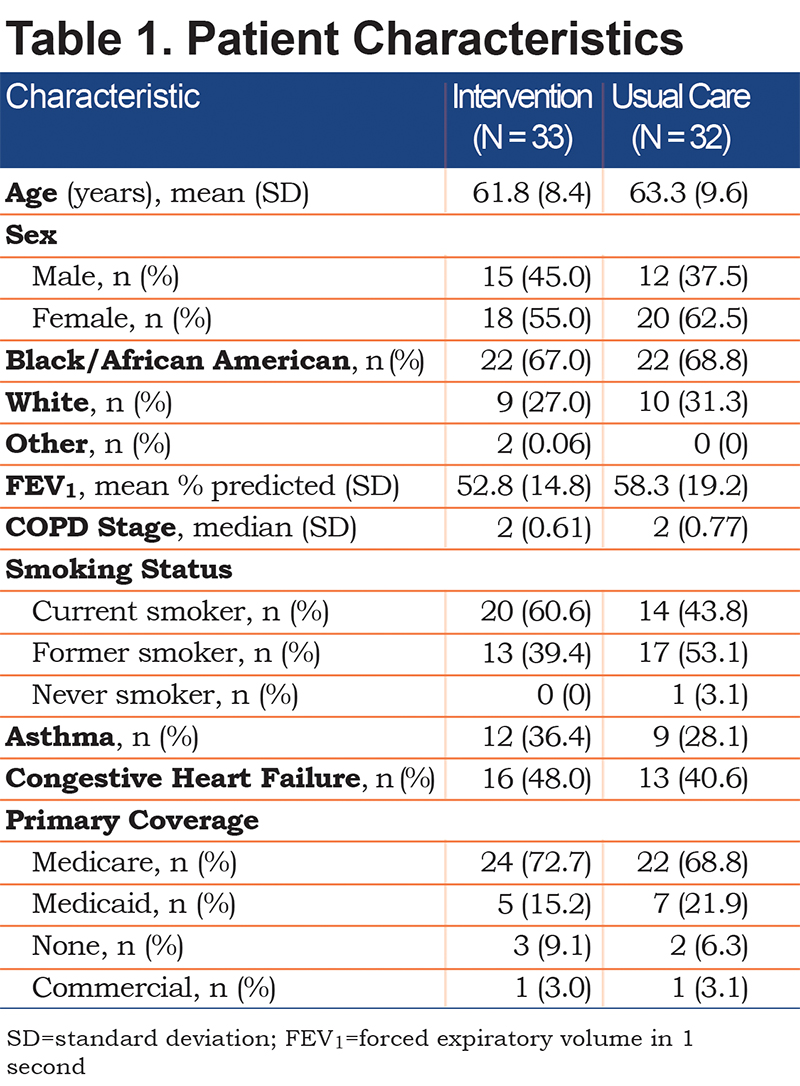
Sixty-five patients were identified with a total of 101 index admissions, and groups were matched according to baseline characteristics (Table 1). The mean age was 62.5 years, approximately 55.3% were female, and 67.7% were Black/African American. The mean forced expiratory volume in 1 second (FEV1) was 60.3% predicted, median stage was 2 based on Global initiative for chronic Obstructive Lung Disease (GOLD),30 about 52% were smokers, 32% had coexisting asthma, and 45% had congestive heart failure.
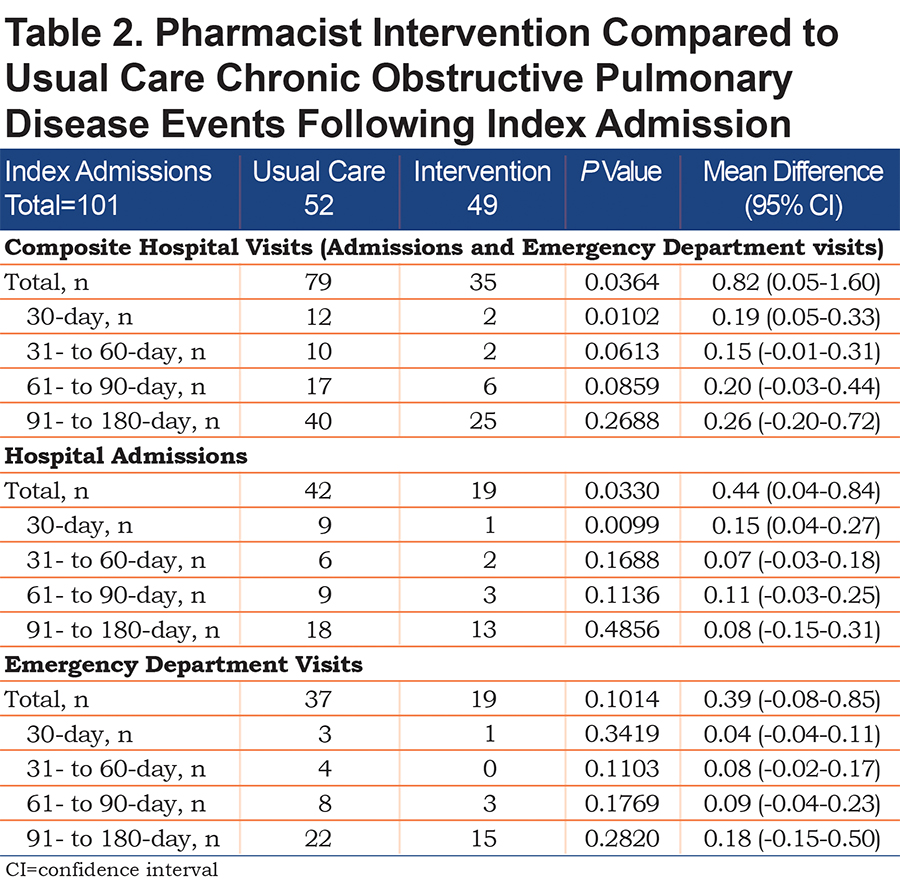
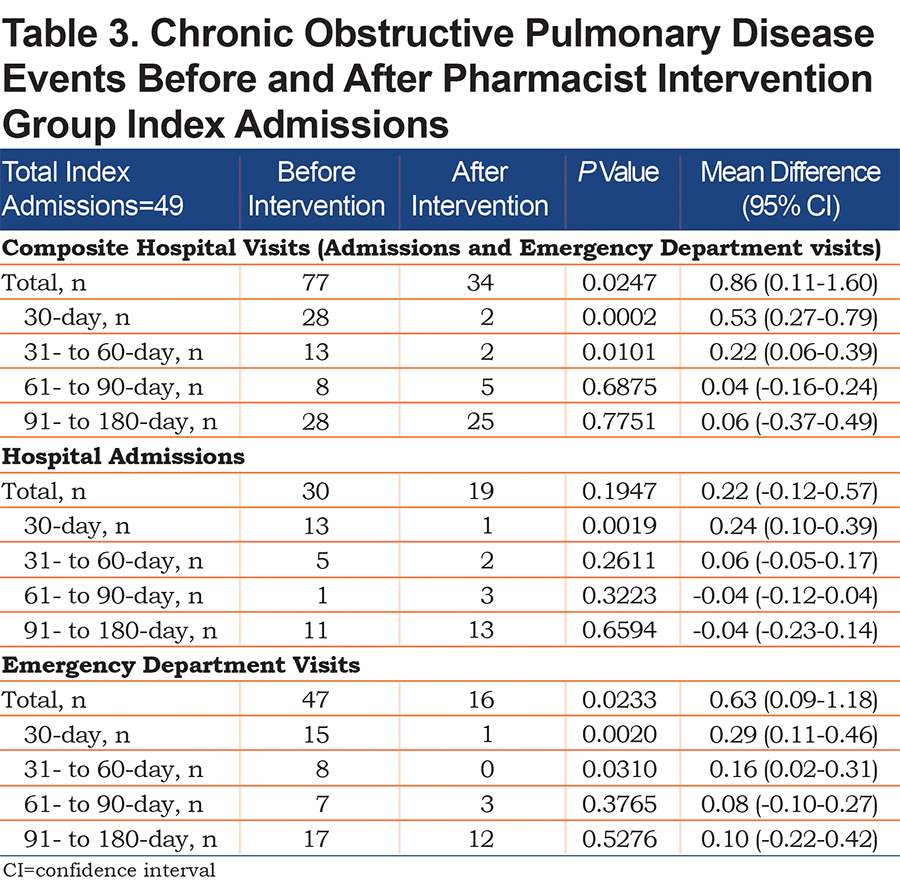
For the primary 180-day composite outcome, significantly less hospital admissions and ED visits were observed with pharmacist intervention compared to usual care (80 versus 35, mean difference 0.82; P=0.0364, 95% CI 0.05-1.60) (Table 2). These outcomes were driven by 30-day hospitalizations (mean difference 0.15; P=0.0099, 0.04–0.27). Additionally, pre-post analysis within the intervention group (Table 3) revealed the primary composite was significantly lower after the intervention compared to before (P<0.0247), driven by 30-day hospitalizations (P=0.0019) and 30- and 60-day ED visits (P=0.0020 and 0.0310, respectively).
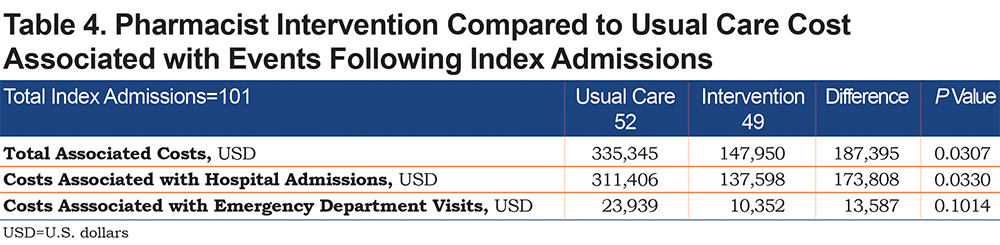
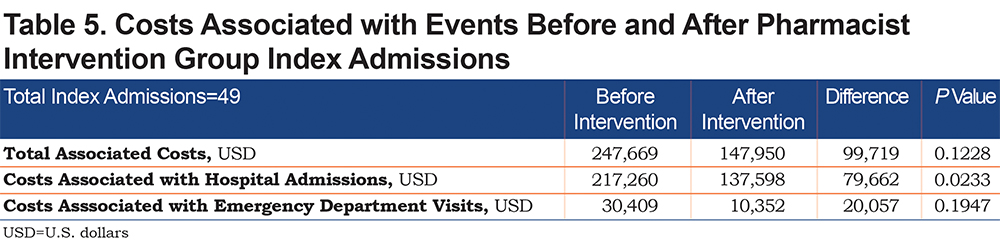
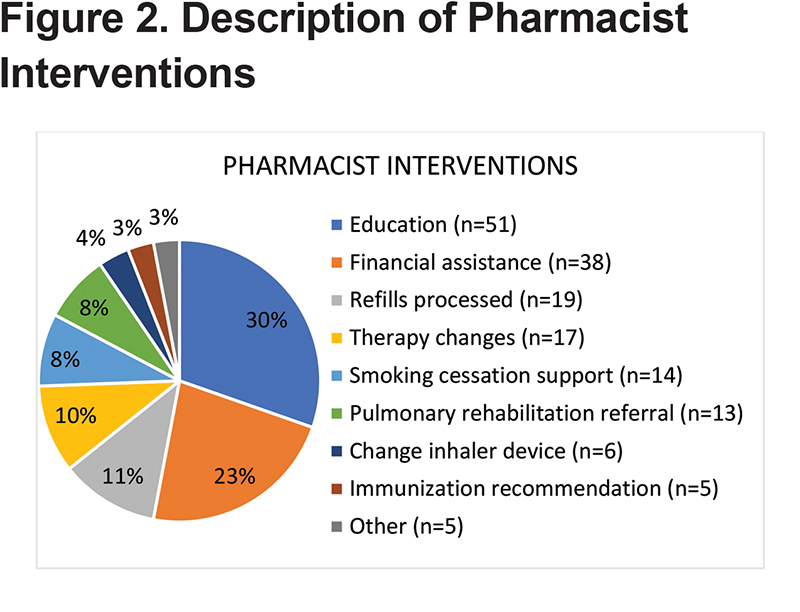
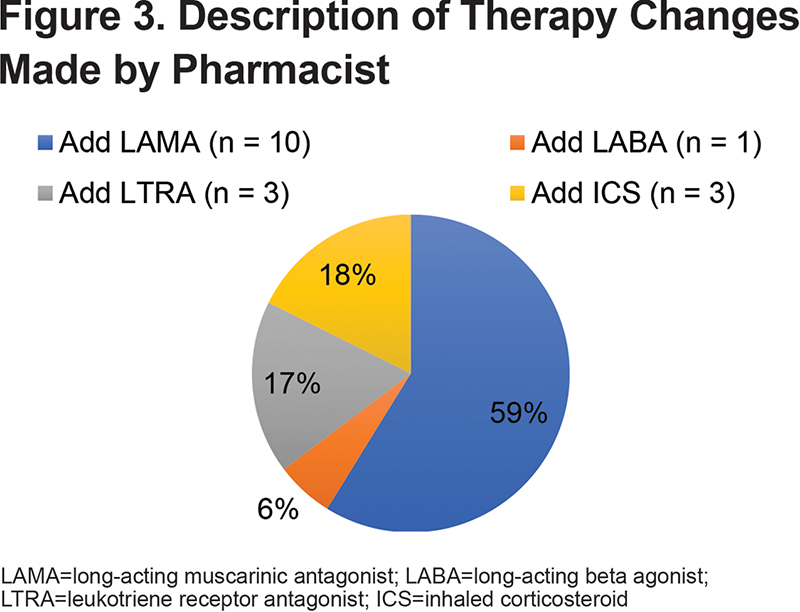
Costs associated with COPD-related hospitalizations was significantly lower in the pharmacist intervention group compared to usual care (mean difference $173,808, P=0.0330) (Table 4), and compared to before intervention (mean difference $79,662, P=0.0233) (Table 5). The most common pharmacist interventions included patient education (30%), medication access assistance (23%), sending refill requests to PCPs (11%), therapy changes (8%), and smoking cessation support (8%) (Figure 2). The most common therapy change (59%) was the addition of a long-acting muscarinic antagonist (LAMA) (Figure 3). Although numerically lower, there were no significant differences between usual care and pharmacist intervention regarding time to follow-up (mean days to phone call 5.3 and 3.0, respectively, P=0.2573; mean days to appointment 18.8 versus 12.7, respectively, P=0.3126) or pneumonia (5 versus 2, respectively, P=0.4378).
Discussion
The comprehensive pharmacist intervention resulted in significantly lower hospital admissions and ED visits. Pharmacists have also demonstrated reduced COPD readmissions in a variety of other settings.9-11 A constellation of interventions with multidisciplinary collaboration can yield the most significant changes, as suggested by Eisenhower.9 Our 30-day pre- and post-hospital admission comparison, a common outcome seen in the literature and associated with significantly increased mortality risk,2,3 resulted in an absolute risk reduction of 22% and a relative risk reduction of 84.6%, exceeding those previously published (Table 6).
We attributed our outcomes to a collation of activities (discharge counseling, medication reconciliation, access and adherence support, and inpatient and outpatient therapy changes), collaboration with team members (physicians, nurses, community pharmacists, social worker, financial counselor, and case managers), and physician acceptance. A similar interprofessional post-discharge service resulted in a 0% readmission rate, although a pre/post comparison was not elucidated.24 Linking community pharmacists to inpatient pharmacists and other team members, and inclusion of other disciplines such as respiratory therapy, have also demonstrated reduced hospital readmissions.31-35 Focusing on medication adherence can have a substantial impact, as inhaler adherence rates may be as low as 10%-40%.36
Regarding other health system interventions which may have impacted our findings, another COPD transitions of care program demonstrated reduced readmission rates from 62% to 41%, a 33.9% relative risk reduction.37 However, this program disbanded prior to initiation of our pharmacist transitions of care service. Upon review, we found no patient in our study enrolled in this program. To our knowledge, no new hospital COPD initiatives were implemented during the study. Other services could have blunted outcomes; still, we found some outcomes to be statistically significant as described above. This suggests that adding pharmacist intervention to standard care, or on top of or integrated into quality improvement initiatives, can further improve care---the aforementioned impact of multidisciplinary collaboration advocated by Eisenhower.9
Between-group outcomes beyond 30 days, and pre/post outcomes beyond 60 days were not statistically lower in our study. It is possible that more frequent follow-up should occur. For instance, after the first post-discharge PCP visit, we followed up every 1 to 6 months. Perhaps following up monthly or every 1 to 3 months would have a significant impact. Outcomes beyond 30 days were numerically lower and, therefore, could be clinically and financially meaningful. We also had a small sample size. A larger population can be sampled by expanding services throughout the health system or to other institutions, including other high-risk conditions, and dedicating more time or personnel.
The clinical pharmacist activities evolved during the time of the study, from placing recommendations initially, to implementing therapy changes using shared decision-making with team and patient discussion (clinical pharmacist practitioner license obtained in 2016). In 2017, the pharmacist was approved by the medical director to automatically refer patients to pulmonary rehabilitation and became involved in teaching pulmonary rehabilitation medication education classes. Other pharmacist activities included primary care clinic visits, teaching and administrative duties, and quality initiatives. Therefore, the pharmacist capture rate varied over time and was difficult to monitor (estimated around 50%-80% during the study). We also did not capture patients with hospital visits in other health systems. Also, the pharmacist only intervened with patients who were admitted to the hospital rather than those who visited the ED without hospitalization. Some patients were not admitted to the hospital long enough for pharmacist identification. In 2019, the pharmacist implemented a new process to capture all patients who visit the hospital for COPD.
In 2017, the GOLD refined ABCD grouping such that pharmacotherapy recommendations are based on exacerbation history and symptoms, irrespective of spirometry.30 Patients hospitalized with 1 or more COPD exacerbations in the past year are recommended to be on at least a LAMA. The preferred next step is to add a long-acting beta2-agonist (LABA). Inhaled corticosteroids may be combined with LABA or LAMA+LABA therapy for patients with elevated blood eosinophils, ongoing symptoms, or exacerbations (2 or more, or 1 hospitalization, per year). There were also new inhalers approved by the Food and Drug Administration during the time of our study. The pharmacist used the most recent guidelines and considered the new inhalers, which may have facilitated practice change in the intervention group.
As in our population, minorities and patients of lower socioeconomic status are disproportionately affected by COPD, challenging hospitals with higher readmission rates and penalties from CMS.38 Specific socioeconomic factors listed in the literature include Medicaid insurance, low income, smoking, non-adherence to medications, and poor literacy. Compounding these challenges is the lack of resources supporting indigent care. These populations may stand to benefit most from pharmacist integration.
The cost analysis was based on previous literature8 indicating simple admissions are estimated to be $7,242. Some of the admissions in our study may have been considered complex, and cost may have been underestimated in these instances. Considering inflation and the potential that some of our admissions may have been complex, our cost estimates are relatively conservative. The associated cost reduction was approximately $62,465 per year and comprised a portion of the pharmacist position, which is a co-funded clinical faculty role. Extrapolating these findings can justify full-time positions focused on transitions of care.
Although direct revenue from pharmacist billing was not monitored in our study, institutions can pursue transitions of care remuneration using various methods. Post-discharge phone calls, clinic appointments, and telephone follow-up are reimbursable ambulatory care services (e.g., transitions of care management, clinic visits, chronic care management). The National Committee for Quality Assurance includes post-discharge medication reconciliation as a performance metric in the Healthcare Effectiveness Data and Information Set.39 Patient satisfaction can influence the Hospital Consumer Assessment of Healthcare Providers and Systems survey, which is a component of the Medicare Hospital Value-Based Purchasing program.40 Inhaler prescriptions and vaccines may increase revenue and medication therapy management claims in the community pharmacy setting. Adherence rates may also be measured.41,42 Ultimately, these activities help to avoid Medicare HRRP readmission penalties, which may correlate to hundreds of thousands of dollars depending on the size of the organization. We selected outcomes based on data accessible to investigators and encourage others to adapt outcomes pertinent to their setting.
Conclusions
The comprehensive and collaborative pharmacist transitions of care service for COPD patients significantly reduced 30-day COPD-related hospital readmissions, ED re-visits, and associated costs in an underserved population.
Acknowledgements
Author contributions: JK was responsible for the conceptualization, design, implementation, data collection and analysis, manuscript development, edits, and manuscript submission. AL was responsible for the conceptualization, design, institutional review board approval, implementation, data collection and analysis, author collaboration and management, manuscript development, edits, and manuscript submission. RA was responsible for the conceptualization, data collection and analysis, manuscript development and editing, and author collaboration.TM was responsible for the conceptualization, implementation, data collection, and manuscript development and edits. CW was responsible for the conceptualization, implementation, and manuscript development and edits.
Declaration of Interest
The authors have no conflicts of interest or financial relationships to disclose.