Running Head: Food Insecurity in COPD
Funding: Comparing Urban and Rural Effects of Poverty on COPD (CURE COPD) was supported by a National Institute on Minority Health and Health Disparities grant P50MD010431 (NNH) and an Environmental Protection Agency grant EPA83615001 (NNH). DCB was supported by an American Lung Association Catalyst Award #942132.
Date of Acceptance: October 18, 2023 | Published Online Date: November 6, 2023
Abbreviations: %pred=percentage predicted; BMI=body mass index; CAT=COPD Assessment Test; COPD=chronic obstructive pulmonary disease; CURE COPD=Comparing Urban and Rural Effects of Poverty on COPD Study; FEV1=forced expiratory volume in 1 second; FVC=forced vital capacity; HADS=Hospital Anxiety and Depression Scale; HADS-A=HADS Anxiety; HADS-D=HADS Depression; HFIAS=Household Food Insecurity Access Scale; ICS=inhaled corticosteroid; IQR=interquartile range; IRR=incident rate ratio; LABA=long-acting beta2-agonist; LAMA=long-acting muscarinic antagonist; mMRC=modified Medical Research Council dyspnea scale; PSS=Perceived Stress Scale; SD=standard deviation; SES=socioeconomic status; SGRQ=St George’s Respiratory Questionnaire
Citation: Belz DC, Woo H, Jackson MK, et al. Food insecurity is associated with COPD morbidity and perceived stress. Chronic Obstr Pulm Dis. 2024; 11(1): 47-55. doi: http://doi.org/10.15326/jcopdf.2023.0440
Online Supplemental Material: Read Online Supplemental Material (148KB)
Introduction
Social determinants of health, such as socioeconomic status (SES), economic instability, and exposure to indoor and outdoor pollutants, have a significant impact on the health of individuals with chronic obstructive pulmonary disease (COPD),1 including higher prevalence of COPD and worse COPD outcomes.2,3 Among the mechanisms by which SES may contribute to health disparities, there is increasing evidence regarding the contribution of dietary factors to respiratory health among individuals with COPD. Specifically, adverse dietary patterns, often common in low SES settings and including diets high in processed and calorie-dense foods but deplete in nutrients or diets low in omega-3 fatty acid intake, have been linked to COPD morbidity.4-9 Food insecurity, or the lack of consistent access to enough food for an active, healthy life, is among the factors that can impact health among low SES individuals.10,11 However, its role in respiratory health in COPD is unclear.
Food insecurity has been associated with cardiometabolic conditions such as hypertension, diabetes, and coronary heart disease in large cross-sectional studies, as well as the development and poor control of diabetes in longitudinal studies.12,13 Possible mechanisms by which food insecurity may impact COPD morbidity include poor dietary quality as well as psychological factors such as stress, anxiety, and depression, which have been associated with food insecurity and separately with COPD morbidity.14-16 Furthermore, since 2007, food insecurity has more than doubled among older adults in the United States,17 the population with the highest prevalence of COPD. In spite of this, limited research has examined whether there is an association between food insecurity and COPD outcomes.
We sought to evaluate the association between food insecurity and COPD morbidity among individuals enrolled in the urban arm of the Comparing Urban and Rural Effects of Poverty on COPD (CURE COPD), a prospective cohort study assessing the impact of air pollution and diet on low-income COPD patients residing in Baltimore. We additionally sought to evaluate the possible association of food insecurity with measures of psychological well-being.
Methods
Study Population and Study Design
Participants were longitudinally followed as part of an observational cohort of former smokers being studied for the impact of diet and indoor air pollution on COPD, with clinic visits at baseline, 3 months, and 6 months and with monthly telephone interviews for the 6-month study period and an additional 3 months after that. Eligible participants were aged 40 or older with physician-diagnosed moderate-to-severe COPD based on a spirometry test (postbronchodilator forced expiratory volume in 1 second [FEV1] to forced vital capacity [FVC] ratio < 0.7 and FEV percentage predicted[%pred] < 80%), a smoking history of >10 pack years, and residing in census tracts with poverty rates above 10% (see the online supplementfor detail). Exclusion criteria are available in the online supplement. Participants were recruited via several methods: (1) a database of participants from prior studies who indicated interest in participation in future studies, (2) recruitment from clinics, including direct physician referral, messages to patients with desired International Classification of Diseases codes, and pulmonary clinic patients who had signed waivers for research contact, (3) flyers posted in outpatient clinics and community locations, (4) social media, newspaper, and radio advertisements, and (5) referral from existing study participants. The study protocols were reviewed and approved by the Johns Hopkins School of Medicine Institutional Review Board, and written informed consent was obtained from all participants prior to any data collection.
Demographic and Socioeconomic Data
Demographic data, including self-reported race, household income, and educational attainment were obtained via questionnaire at baseline. Information on neighborhood characteristics was obtained via geocoded address at baseline. Limited neighborhood food access was defined as an area where at least a third of people live more than 0.5 miles from the nearest supermarket, supercenter, or large grocery store in urban areas (or more than 10 miles in the case of rural areas).18 Neighborhood poverty rate represented the percentage of all families in a census tract with annual income below the federal poverty rate.19
Food Insecurity Assessment
The Household Food Insecurity Access Scale (HFIAS) is a validated metric used for measuring a household-level state of food security20 – defined as a state in which “all people [in the household] at all times have both physical and economic access to sufficient food to meet their dietary needs for a productive and healthy life.”10 The instrument consists of 18 questions: 9 questions on occurrence (yes/no), with each having a single follow-up question on frequency—that assesses whether households are food secure or insecure based on a participant’s 30-day recall of his/her household experience (see the online supplement for detail). For our study, the HFIAS questionnaire was administered by trained staff at each clinic visit – baseline, 3-month, and 6-month.
Along with the overall food insecurity measure, 3 subdomains of the HFIAS were also explored: (1) anxiety and uncertainty about food supply, (2) insufficient food quality, and (3) insufficient food intake and its physical consequences.
Respiratory Outcomes
Validated respiratory outcome measures were assessed by trained staff longitudinally at each clinic visit. Medication use was assessed by participant self-report via questionnaire. Health status was assessed with the COPD Assessment Test (CAT),21 dyspnea was assessed with the modified Medical Research Council (mMRC) scale,22 and respiratory-specific quality of life was assessed with the St George’s Respiratory Questionnaire (SGRQ).23 In addition, exacerbation data was prospectively monitored over 9 months with monthly telephone interviews. Moderate exacerbations were defined as an unscheduled doctor’s visit, antibiotic or systemic steroid use, or treatment in an urgent care facility due to COPD-related illness. Severe exacerbations were defined as any COPD-related emergency department visit or hospitalization. Spirometry was performed according to the American Thoracic Society protocol24 (Koko spirometer, Nspire Health Inc.) at each study visit.
Assessment of Psychological Well-being
Symptoms of depression and anxiety were assessed at each visit via the 14-question Hospital Anxiety and Depression Scale (HADS)25 which has 2 subscales, HADS-Anxiety (HADS-A) and HADS-Depression (HADS-D). Stress was assessed via the Perceived Stress Scale (PSS), a 10-item self-report questionnaire designed to measure “the degree to which individuals appraise situations in their lives as stressful.”26
Statistical Analysis
Baseline participant characteristics were summarized using mean (standard deviation [SD]) or median (interquartile range [IQR]) for the continuous variables and frequency (%) for the categorical variables. Due to a large majority of participants reporting as food secure at each visit (approximately>85%), the primary analysis used HFIAS as a categorical indicator with 2 categories: food secure at all times or ever food insecure during the study period. Per guidelines,20 the dichotomous indicator (secure versus insecure) was constructed for each subdomain of the HFIAS food insecurity indicator, and similar to the overall indicator, the subdomain indicators were treated as categorical: secure at all times or ever insecure during the study period.
To assess the associations between respiratory morbidity and food insecurity, we conducted linear regression of continuous COPD outcomes on dichotomous food insecurity, using generalized linear mixed models to account for the repeated measures, adjusted for covariates. For the total frequency of exacerbations across the study period, negative binomial regression of exacerbations was conducted with the dichotomous indicator of food insecurity and the participant’s total follow-up days as an offset, adjusted for covariates in the parsimonious and primary models. The parsimonious model included individual factors of baseline age, gender, race, smoking pack years, body mass index (BMI), comorbidity count,27 controller medication use, and FEV1 %pred based on the Global Lung Function Initiative race-neutral spirometry equation.28,29 The primary model included all covariates of the parsimonious model and added the individual and neighborhood SES factors of educational attainment, household income, neighborhood poverty rate, and limited neighborhood food access.
As secondary analyses, we repeated the main regression of COPD morbidity with the subscales of the HFIAS: (1) anxiety and uncertainty about food supply, (2) insufficient food quality, and (3) insufficient food intake and its physical consequences, and separate regression analyses were run for each. We further explored the association of food insecurity with depressive and anxiety symptom scores (HADS-D/A) and the PSS as secondary outcomes.26
Missing observations for covariates were few and were imputed using sample means. All analyses were conducted with Stata/IC 15.1 software (Stata Corp, College Station, Texas), and statistical significance criteria were set at p<0.05.
Results
Study Population Characteristics
A total of 116 individuals were recruited into the study, with 17 withdrawing before all baseline data could be collected. Ninety-nine individuals completed the baseline visit between 2016 and 2021 and had available data regarding food access and respiratory morbidity, which comprises the entire urban cohort of the CURE COPD study. The average age of the study population was 66.4 years, 55% of participants were female, and 41% were White (Table 1). Participants had smoked an average of 46.3 pack years and the mean FEV1%pred was 49.8. Approximately half of the participants (49%) had educational attainment of high school education or less, and two-thirds (66%) had an annual household income of less than $30,000, representing an overall low-income population.
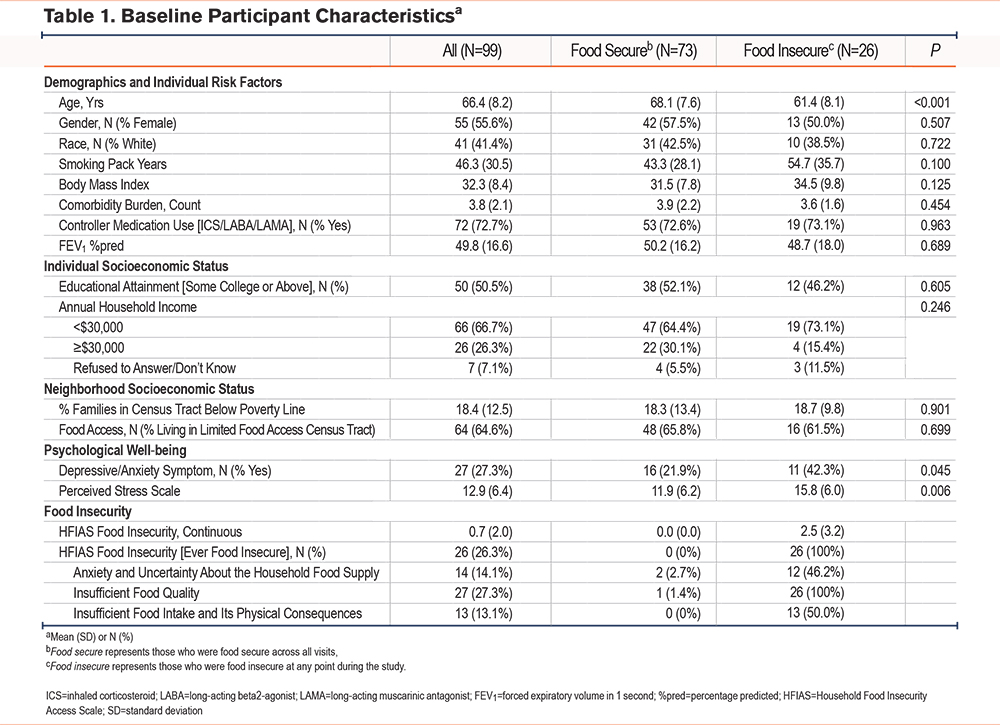
A total of 26.3% of participants were ever food insecure during the study. Of those individuals reporting food insecurity, 12 (46%) reported anxiety and uncertainty about household food supply, 26 (100%) reported insufficient food quality, and 13 (50%) reported insufficient food intake with physical consequences. Compared to participants who were always food secure, participants who were ever food insecure were younger (61 versus 68 years old), more likely to report depressive or anxiety symptoms (42% versus 22%), and had higher perceived stress.
Associations Between Food Insecurity and COPD Morbidity
In the parsimonious model, adjusting for baseline demographic and clinical factors, food insecurity was associated with a higher incidence rate of moderate and severe exacerbations during the study period (IRR=2.2, p=0.031). Food insecurity was also associated with a worse COPD health status (higher CAT score: β=2.7, p=0.044), worse dyspnea (higher mMRC score: β=0.5, p=0.002), and a worse respiratory-specific quality of life (higher SGRQ score: β=6.4, p=0.039) (Table 2).
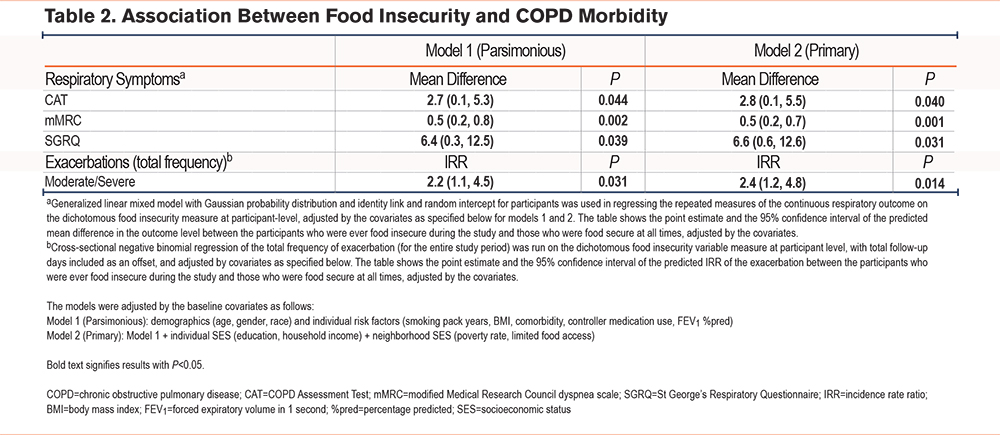
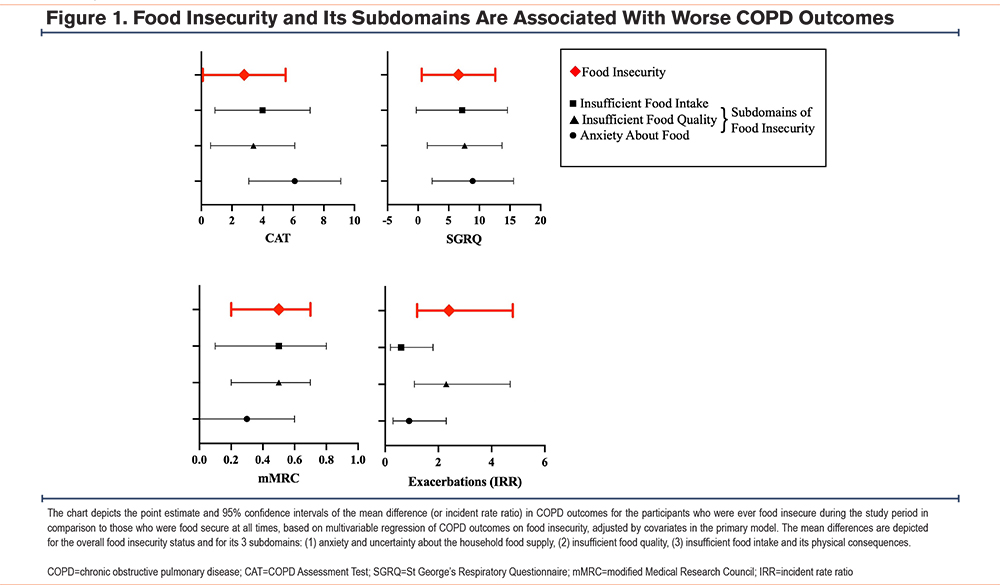
In the primary model, after additionally adjusting for individual SES, neighborhood poverty, and low healthy food access, the association of food insecurity with respiratory outcomes was robust. Specifically, food insecurity continued to be associated with a higher incidence rate of moderate and severe exacerbations during the study period (IRR=2.4, p=0.014). Food insecurity was also associated with worse COPD health status (higher CAT score: β=2.8, p=0.040), worse dyspnea (higher mMRC score: β=0.5, p=0.001), and worse respiratory-specific quality of life (higher SGRQ score: β=6.6, p=0.031) (Table 2, Figure 1).
Secondary Analyses
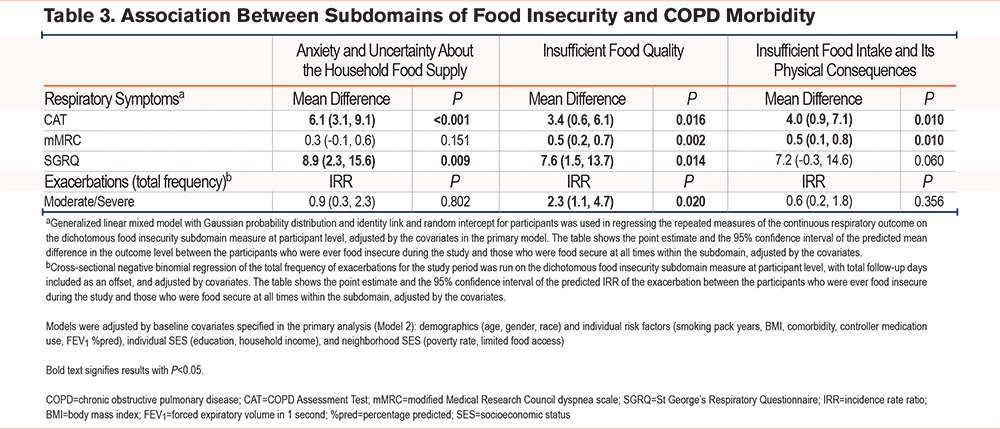
Among subdomains of food insecurity, reported insufficient food quality was associated with all measured outcomes, including a higher incidence rate of moderate and severe exacerbations during the study period and worse CAT, mMRC, and SGRQ. Reported insufficient food intake was associated with patient-reported outcomes of worse CAT and mMRC scores (Table 3, Figure 1). Anxiety and uncertainty about food supply were associated with worse CAT and SGRQ scores.
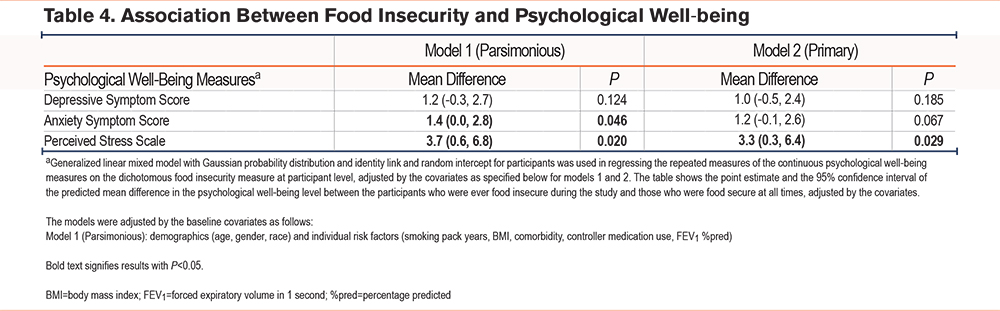
In the parsimonious model, food insecurity was associated with increased depressive symptoms, increased anxiety symptoms, and increased perceived stress (Table 4). This association remained robust for perceived stress after adjustment for individual and neighborhood SES factors and neighborhood food access in the primary model (β=3.3, p=0.029), although the association of depressive symptoms and anxiety symptoms with food insecurity was no longer statistically significant.
Discussion
This prospective observational study of urban, low-income former smokers with COPD demonstrates an association between food insecurity and respiratory morbidity. Specifically, those reporting food insecurity during the study had an increased incidence of moderate and severe COPD exacerbations and worse dyspnea, COPD health status, and respiratory-specific quality of life. These findings add to the growing body of literature regarding social determinants of health and COPD morbidity and mechanisms by which socioeconomic disadvantage worsens COPD outcomes.
There are numerous mechanisms by which SES can impact respiratory health, including increased exposure to indoor and outdoor pollution as well as lack of access to health care.1,30 Among these multiple possible mechanisms, the current study provides evidence that food insecurity has an independent association with COPD morbidity. Even when adjusting for other markers of SES, including education level, individual and neighborhood income, and neighborhood access to healthy food, food insecurity continues to have a significant association with exacerbations and patient-reported outcomes.
Analyses of the subdomains of food insecurity and measures of psychological well-being support a complex influence of food insecurity on respiratory morbidity in COPD (Figure 1). Levels of perceived stress have been associated with increased health care utilization among individuals with COPD,15 and stress may directly influence COPD pathophysiology through chronic inflammation.31 The state of food insecurity and anxiety surrounding it may impact symptoms. Indeed, the subdomain of food insecurity related to anxiety and uncertainty about food supply was associated with worse health status and quality of life. Furthermore, perceived stress was significantly associated with food insecurity.
Additionally, the subdomain of food insecurity related to food quality was associated with increased exacerbation rates and worse patient-reported outcomes. This suggests that the actual quality of diet plays a direct role in COPD morbidity independent of the stress of food insecurity or the other mechanisms of socioeconomic health disparities. Low-quality diets as assessed via the Alternative Healthy Eating Index and characteristic of low intakes of fruit, vegetables, omega-3 fatty acids, and whole grains, have been shown to be associated with an increased risk of developing COPD.9,32-34 Similarly, “Western” diets high in refined grains, red and processed meats, and soft drinks have been associated with respiratory morbidity including the prevalence of COPD.35 In addition to overall dietary quality, specific nutrient intakes have also been associated with respiratory disease. In particular, diet quality may impact respiratory health through antioxidants and anti-inflammatory mediators such as omega-3 fatty acids, 36,37 which may reduce the chronic inflammation that is the hallmark of COPD progression.38-40
Among the strengths of this study is the extensive clinical and socioeconomic data collected on participants. This allows for the differentiation of the various possible mechanisms by which SES and comorbidities may influence COPD outcomes. The study population is enriched for low-income individuals living in an urban environment and accordingly is representative of the specific challenges of such an environment. For instance, the percentage of participants reporting food insecurity within a 6-month period (26%) was substantially higher than the national rate of food insecurity during a given year (10%).41 The small size of the study and specific socioeconomic inclusion criteria could limit the overall generalizability of the study but emphasize the importance of social determinants of health in this population. Finally, while analysis of food insecurity subdomains suggests diet quality could play a direct role in COPD morbidity, further studies with measures of general diet quality are needed to determine the role of diet quality in COPD.
Conclusion
This study of former smokers with COPD living in urban Baltimore found a significant association between food insecurity and respiratory morbidity. Individuals who experienced food insecurity during the study had a higher incidence of moderate or severe COPD exacerbations and worse health status, dyspnea, respiratory-specific quality of life, and perceived stress. These associations persisted even when adjusting for other socioeconomic factors such as education level as well as individual and neighborhood income and neighborhood food access. Additionally, subdomains of food insecurity were individually associated with respiratory morbidity. These findings suggest that food insecurity may be one of the contributors to socioeconomic disparities in COPD.
Acknowledgements
Author contributions: DB and NH provided study conceptualization, HW provided data analysis, WL provided study investigation and project administration, MM was responsible for resources, CH and NH were responsible for methodology and NH was responsible for funding acquisition with NP, MM, CH, and NH providing supervision. DB wrote the manuscript’s original draft and HW, MJ, NP, AF, MM, ME, CH, and NH contributed to the manuscript’s writing, review, and editing. All authors approved the manuscript for publication.
Declaration of Interests
Daniel Belz reports grants from the National Institutes of Health (NIH)/National Heart, Lung, and Blood Institute (NHLBI) and the American Lung Association and grants and personal fees from Insmed Incorporated. Nirupama Putcha reports grants from the NIH/National Institute of Environmental Health and the NHLBI and personal fees from Regeneron and GSK. Ashraf Fawzy reports grants from the NIH/NHLBI and personal fees from Regeneron during the conduct of the study. Meredith McCormack reports grants from the NIH/NHLBI and personal fees from GSK. Michelle Eakin reports grants from the NIH/NHLBI. Nadia Hansel reports grants from the NIH, Environmental Protection Agency, and the COPD Foundation, grants and personal fees from AstraZeneca, grants and personal fees from GSK, grants from Boehringer Ingelheim, and personal fees from Mylan.