Running Head: Plasma Omega-3 Levels Associated With COPD Morbidity
Funding Support: The study, Comparing Urban and Rural Effects of Poverty on COPD (CURE COPD), was developed under Assistance Agreement No. 83615001 awarded by the U.S. Environmental Protection Agency (EPA). It has not been formally reviewed by the EPA. The views expressed in this document are solely those of the authors and do not necessarily reflect those of the Agency. The EPA does not endorse any products or commercial services mentioned in this publication. Research reported in this publication was supported by the National Institute on Minority Health and Health Disparities of the National Institutes of Health (NIH) under award number: P50MD01043 and grants from the NIH (NIH F32 ES029789-01A1).
Date of Acceptance: April 15, 2024 | Publication Online Date: April 22, 2024
Abbreviations: ALA=α-linolenic acid; BMI=body mass index; CAT=COPD assessment test; CI=confidence interval; COPD=chronic obstructive pulmonary disease; DHA=docosahexaenoic acid; DPA=docosapentaenoic acid; EPA=eicosapentaenoic acid; FEV1=forced expiratory volume in 1 second; FEV1%pred=forced expiratory volume in 1 second percentage predicted; FVC=forced vital capacity; GLMM=generalized linear mixed model; ICC=intraclass correlation; IFN=interferon; IL=interleukin; MaR1=Maresin-1; mMRC=modified Medical Research Council; OR=odds ratio; PKC=protein Kinase C; PMN=polymorphonuclear leukocytes; PUFA=polyunsaturated fatty acid; SD=standard deviation; SGRQ=St George’s Respiratory Questionnaire; SPMs=specialized pro-resolving mediators; TNF=tumor necrosis factor
Citation: Kemper TA, Woo H, Belz D, et al. Higher plasma omega-3 levels are associated with improved exacerbation risk and respiratory-specific quality of life in COPD. Chronic Obstr Pulm Dis. 2024; 11(3): 293-302. doi: http://doi.org/10.15326/jcopdf.2023.0468
Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of death in the United States1 and is widely acknowledged to be associated with factors such as tobacco smoking and exposure to various irritant particles and gases.2,3 There is growing awareness of the significant impact of dietary intake on respiratory health.4,5 In particular, polyunsaturated fatty acids (PUFAs) are an essential source of biologically active lipid-derived anti-inflammatory and pro-resolving mediators such as resolvins, maresins, and protectins.6 These pro-resolving mediators, which may act on chronic, unrestrained pulmonary inflammation, are primarily derived from omega-3 fatty acids, such as plant-sourced α-linolenic acid (ALA) or fish-sourced eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA)7,8—and to a lesser well-known degree, docosapentaenoic acid (DPA).9,10 Previous studies have illuminated the therapeutic potential of omega-3 PUFAs in conditions such as cardiovascular disease and inflammatory bowel diseases.11,12 Most research investigating the relationship between omega-3 PUFAs and respiratory disease, particularly COPD, has primarily focused on subjectively measured omega-3 intake based on participants' self-reported dietary intake, suggesting an association between EPA and DHA intake and COPD morbidity.13-15 Limited studies have adopted a more objective approach to investigating the impact of blood omega-3 PUFA concentrations on COPD morbidity. Shahar et al found the prevalence of COPD inversely related to the DHA concentration in plasma lipids, suggesting that the fatty acid may have preventative and protective properties in current and former smokers.16 Similarly, Patchen et al observed higher circulating omega-3 fatty acids, especially DHA, were associated with attenuated lung function decline and decreased odds of airway obstruction.17 Our study advances the investigation of these relationships by utilizing objective blood-based biomarkers to observe whether plasma concentrations of omega-3 fatty acids, specifically EPA and DHA, are associated with respiratory outcomes in former smokers with moderate-to-severe COPD. By focusing on objective biomarkers, this research seeks to further elucidate the impact of dietary intake of these omega-3 fatty acids on COPD morbidity, highlighting the role of nutritional factors in respiratory health and their potential in managing COPD.
Methods
Study Population and Design
This observational, 6-month prospective study utilized data from the first 57 participants who completed all visits from the urban cohort of the Comparing Urban and Rural Effects of Poverty on COPD (CURE COPD) study. The Johns Hopkins Medical Institutional Review Board approved the study (IRB00069904), and all participants provided written informed consent before beginning the study. Participants were from low-income communities in Baltimore, Maryland, who met the inclusion criteria of: (1) 40 years or older; (2) a postbronchodilator forced expiratory volume in 1 second (FEV1)/ forced vital capacity (FVC) less than 0.70; (3) an FEV1 percentage predicted (FEV1%pred) less than 80%; and (4) a former smoker (self-reported at least 6-months of smoking cessation and exhaled carbon monoxide ≤ 6 ppm18 with at least a 10 pack-year history of tobacco use). Participants were followed at in-person study visits every 3 months (baseline, 3 months, and 6 months). Demographics, smoking history, and comorbidity were assessed by questionnaire.
Plasma Omega-3 Fatty Acid Analysis
Plasma was collected from participants at each study visit. Participants' plasma was analyzed for omega-3 concentrations (EPA, DHA, DPA, ALA) in absolute scale (μg/mL) using the gas chromatography/mass spectrometry method.19
Respiratory Health Outcomes
At each study visit, questionnaires were administered, including the COPD assessment test (CAT) (measures the impact of COPD),20 the modified Medical Research Council (mMRC) dyspnea scale (measures functional impairment due to dyspnea),21 and the St George’s Respiratory Questionnaire (SGRQ) (measures respiratory-specific quality of life).22 For the SGRQ, we utilized the total score, which encompasses the overall impact of the disease on health status, including symptoms, activity, and impact components. History of moderate (oral steroid use, antibiotics use, or unscheduled physician visit due to COPD in the last 3 months) and severe exacerbations (emergency department/hospital visits due to COPD in the last 3 months) were assessed by monthly phone calls.
Biomarkers
At each study visit, serum specimens were collected and analyzed in the clinical laboratory within 2 hours of collection, aliquoted, and stored at -80⁰C. Serum biomarkers were measured using the multiplex assay process detailed in Fawzy et al23 and included the following markers of inflammation: tumor necrosis factor (TNF)-α, interleukin (IL)-6, IL-8, and interferon (IFN)-γ.
Statistical Analysis
To evaluate the relationship between plasma omega-3 levels and COPD morbidity, a generalized linear mixed model (GLMM) with a random intercept was employed.24 This model is appropriate for per-measurement data (as opposed to per-patient data) by accounting for nonindependent observations within individuals, and the model adjusted for baseline covariates, including age, gender, race (White versus non-White), education (some college or above versus high school graduate or below), smoking pack years, body mass index (BMI), comorbidity count, FEV1 %pred using race-neutral Global Lung Initiative equations,25 and neighborhood poverty—as represented by the percentage of families living below the poverty line in a census tract.26 Gaussian probability distribution with an identity link function was applied for continuous outcomes (CAT, mMRC, and SGRQ). For dichotomized exacerbation outcomes (severe and moderate), a binomial distribution with a logit link function was used. The analysis obtained the mean difference in continuous outcomes or the odds ratio for exacerbation outcomes per 1 standard deviation (SD) increase in plasma omega-3. As a secondary analysis, the relationship between plasma omega-3 and inflammatory biomarkers (TNF-α, IL-6, IL-8, IFN-γ) was assessed using the same method used for the continuous COPD outcomes; except biomarkers were log-transformed because of their skewed distributions and their associations with plasma omega-3 expressed in terms of percentage change in geometric mean concentrations per 1 SD increase in plasma omega-3. Plasma omega-3 was primarily represented by the sum of EPA and DHA (EPA+DHA), based on prior studies associating EPA+DHA intake via food frequency questionnaire with COPD morbidity.15 To assess the linearity assumption in regression analysis and allow the flexible, functional shape of the association between omega-3 and COPD outcomes, a secondary analysis was also run using restricted cubic spline GLMM regression. The secondary analysis explored various representations of omega-3, including incorporating DPA and ALA as omega-3 (EPA+DHA+DPA+ALA). Additionally, the analysis evaluated EPA, DHA, DPA, and ALA separately, as well as expressing omega-3 as a percentage of total fatty acids. All analyses were performed using Stata, version 15.1 (Stata Corp, College Station, Texas). Statistical significance was defined as p < 0.05.
Results
Participant Characteristics
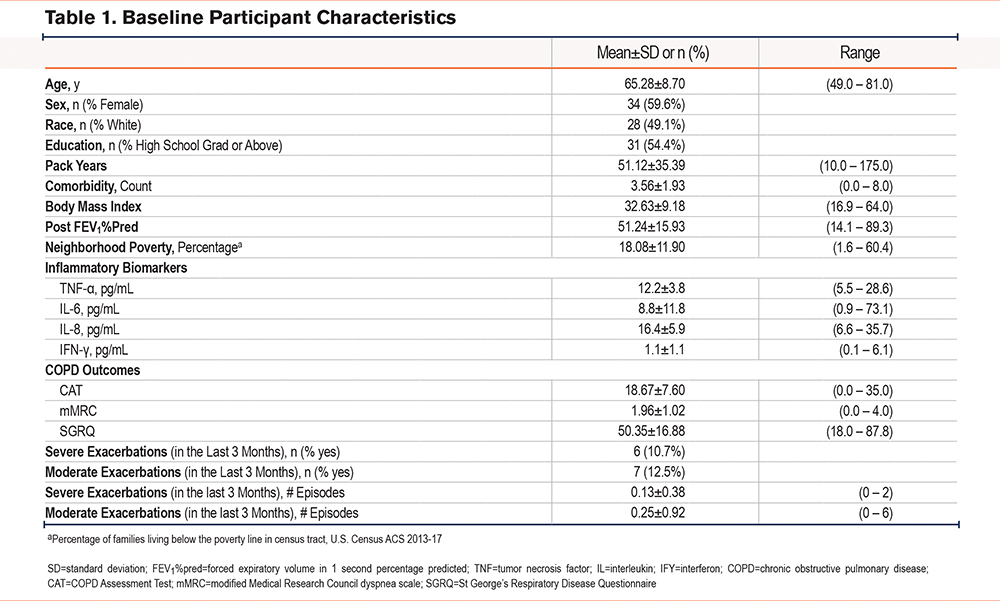
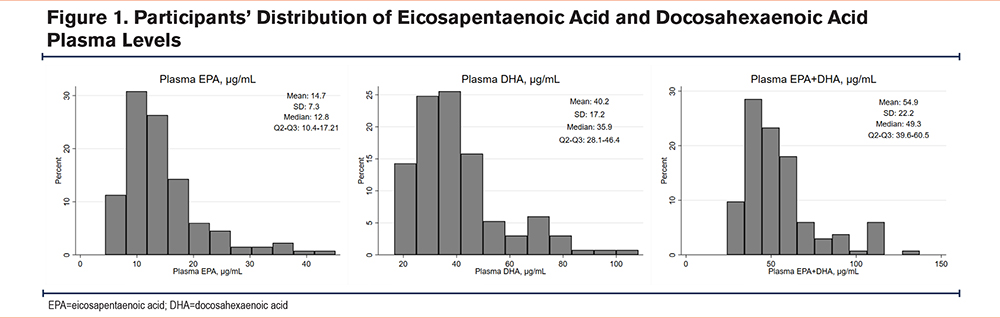
Our study’s 57 participants had a mean (±SD) age of 65.3 years (±8.7) and a mean BMI of 32.6 (±9.2), consisting of 34 females (59.6%) and 28 persons identifying as White (49.1%) (Table 1). Participants had a mean of 51.1 pack years (±35.4) of smoking. Participants reflected a relatively low-income population, with about one-fifth of residents living in neighborhoods below the poverty line (18.1%) and almost half (45.6%) having less than a high school education. Participants had an average of 3 comorbidities (3.6±1.9), moderate-to-severe COPD reflected by a mean FEV1 %pred of 51.2% (±15.9), and patient-reported outcome scores reflecting a moderate COPD health impact.20,27,28 Participants’ mean plasma EPA+DHA levels were 54.02µg/mL (±22.2) with a mean plasma EPA of 14.7µg/mL (±7.3) and mean DHA of 40.2µg/mL (±17.2) (Figure 1). There was also some within-person variability in plasma EPA+DHA, with the intraclass correlation (ICC) of 0.81 and within-person standard deviation of 9.7μg/mL; for EPA, the ICC and within-person SD were 0.71 and 4.0μg/mL, respectively while for DHA 0.81 and 7.5μg/mL. In comparison, the between-person SD of EPA+DHA, EPA, and DHA were 19.8, 6.2, and 15.4μg/mL respectively. Out of 57 participants with plasma omega-3 data, 84% (48 out of 57) had omega-3 measured across multiple visits (28 participants in all 3 visits and 20 in 2 visits), while 9 participants had omega-3 data in just one visit.
Association of Eicosapentaenoic Acid + Docosahexaenoic Acid Levels With COPD Morbidity and Inflammatory Biomarkers
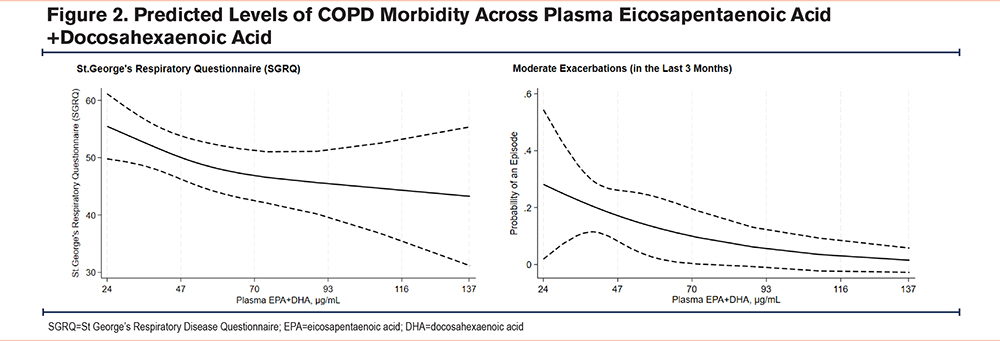
After adjusting for covariates, higher EPA+DHA plasma levels were associated with lower SGRQ and lower risk of moderate exacerbations (Table 2 and Figure 2). Specifically, a 1 SD (~ 22.2µg/mL) increase in EPA+DHA levels was associated with a 2.7 points lower SGRQ score, reflecting better respiratory-specific quality of life (95% confidence interval [CI] -5.2, -0.2; p=0.04). Protective associations of EPA+DHA were also demonstrated for moderate exacerbations, with a 1 SD increase in EPA+DHA levels associated with 60% lower odds of moderate exacerbations (odds ratio [OR] 0.40; 95% CI 0.2, 0.9; p=0.02). Although omega-3 showed a trend towards better COPD metrics for other respiratory health outcomes (i.e., 0.8 points lower CAT [95% CI -2.4, 0.8, p=0.3]) and 30% lower odds of severe exacerbations (OR 0.7; 95% CI 0.3, 1.4, p=0.3), neither reached statistical significance. Plasma EPA+DHA showed no trends with mMRC (p=0.7). The results were similar in sensitivity analyses, which only included participants who had omega-3 data on multiple visits (data not shown).
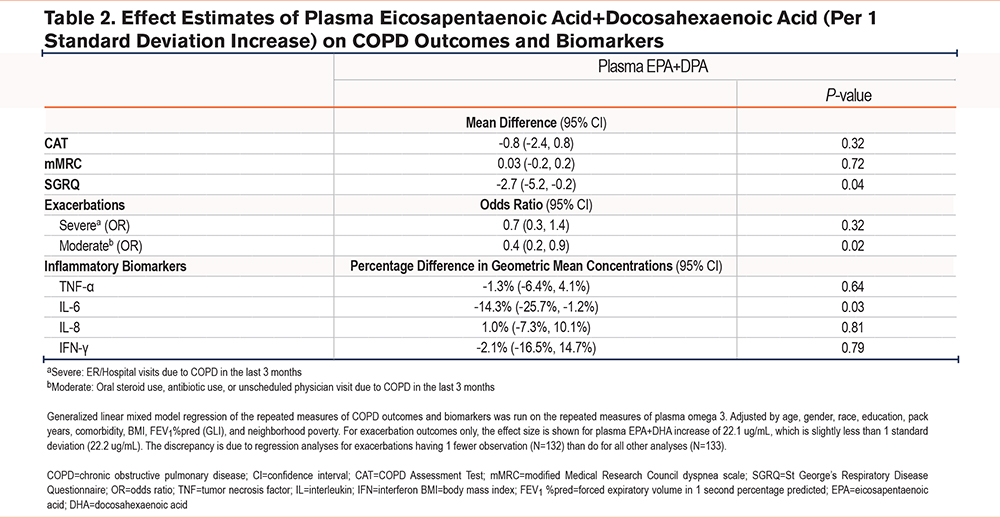
There was also a significant plasma EPA+DHA difference in IL-6 mean concentrations, with higher EPA+DHA plasma levels associated with reduced IL-6 (Table 2). For example, IL-6 mean concentrations were 14.3% lower for those with 1 SD higher plasma EPA+DHA (95% CI 1.2%, 25.7%; p=0.03). However, other markers of inflammation (TNF-α, IL-8, and IFN-γ) did not show associations with plasma EPA+DHA (Table 2).
Association of Total Omega-3 and Isolated Eicosapentaenoic Acid, Docosahexaenoic Acid, Docosapentaenoic Acid, and α-Linolenic Acid With COPD Morbidity and Biomarkers
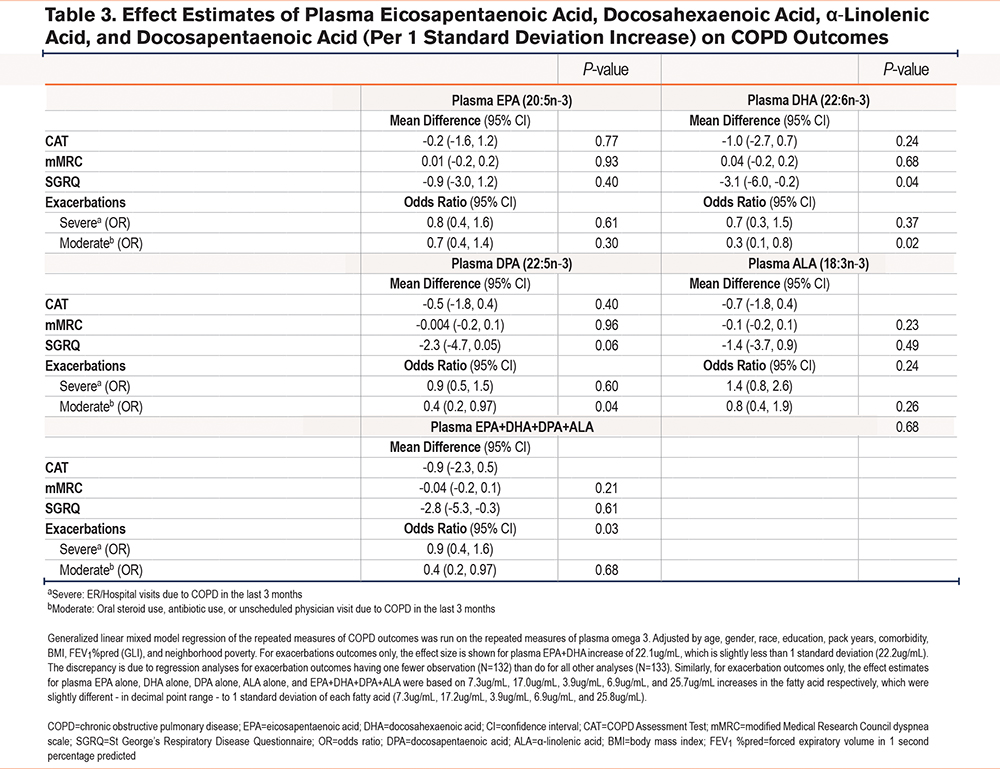
Associations between total omega-3 (EPA + DHA + DPA + ALA) and COPD outcomes were similar to those with EPA+DHA (Table 3). A higher total omega-3 level was associated with a 2.8-point lower SGRQ score (95% CI -5.3, -0.3; p=0.03) and 60% lower odds of moderate exacerbations (CI 0.2, 0.97; p=0.04). The results seem to be primarily driven by DHA, as a 1 SD increase (~ 17.2µg/mL) in DHA levels was associated with a 3.1 lower SGRQ score (95% CI -6.0, -0.2; p=0.04) and 70% lower odds of moderate exacerbations (95% CI 0.1, 0.8; p=0.02). DPA also demonstrated notable associations with these outcomes ([SGRQ; mean difference -2.3; 95% CI -4.7, 0.05, p=0.06], [moderate exacerbations; OR 0.4; 95% CI 0.2, 0.97, p=0.04]) (Table 3). There was no association between EPA or ALA with COPD outcomes. There was no association between omega-3 fatty acids and respiratory outcomes when expressed as a percentage of total fatty acids (data not shown).
The patterns of associations between total omega-3 (EPA + DHA + DPA + ALA) and inflammatory biomarkers were similar to those shown with EPA+DHA. Adjusting for covariates, a higher total omega-3 level was associated with a 15.5% lower IL-6 concentration (95% CI 3.3%, 26.1%; p=0.01), with DHA and DPA suggested as the primary drivers of the association. For example, a 1 SD increase in DHA levels was associated with a 16.1% lower IL-6 concentration (95% CI 2.7%, 27.7%; p=0.02) and a 1 SD increase in DPA with a 14.9% lower IL-6 concentration (95% CI 2.5%,25.7%; p=0.02); however, IL-6 concentrations did not differ by either EPA or ALA. Other inflammatory biomarkers—TNF-α, IL-8, and IFN-γ—did not show associations with either total or individual plasma omega-3; and, when expressed as a percentage of total fatty acids, omega-3 fatty acids did not show associations with any inflammatory biomarkers, including IL-6 (data not shown).
Discussion
This study found that among former smokers with moderate-to-severe COPD, higher plasma omega-3 (EPA+DHA) levels were associated with lower COPD morbidity, specifically better respiratory-specific quality of life and reduced odds of moderate exacerbations. When exploring the association of individual fatty acids with respiratory morbidity, significant associations were particularly noted for DHA and, to a lesser extent, with DPA, as opposed to other measured fatty acids (EPA and ALA). Higher plasma omega-3 (EPA+DHA) levels were also associated with lower IL-6 concentrations, a common marker of systemic inflammation. This study utilizes objectively measured omega-3 levels to add to the emerging evidence about the potential role of diet in lung health and systemic inflammation.
Previous investigations into omega-3 PUFAs' effects on COPD morbidity have primarily relied on subjective measurements based on self-reported dietary intake.13-15,29 Although widely adopted for use in epidemiological studies,30-32 there are notable limitations to participant-reported dietary intake. Dietary intake surveys, by design, are instruments for categorizing participants based on previous dietary intake rather than estimating absolute nutritional intake33 and are subject to reproducibility errors34 and participant bias.35 Previous studies utilizing self-reported dietary intake using food frequency questionnaires suggest that increased dietary intake of omega-3 fatty acids is linked with improved respiratory health, and in particular, lower incidence of bronchitis and emphysema,13 better respiratory-specific quality of life,14 lower odds of respiratory symptoms,15 higher lung function,13 and lower concentrations of serum inflammatory markers.29 Moreover, emerging data indicates that the positive impact of omega-3 consumption on respiratory health may be particularly noteworthy in individuals exposed to deleterious environmental factors like cigarette smoke exposure,15 thereby, contributing additional evidence to underscore the significance of omega-3 PUFAs in influencing COPD health outcomes.
By utilizing objective plasma markers of omega-3 PUFAs, our findings contribute valuable insights into the potentiation of supplements and dietary modifications to regulate the effects of specialized proresolving mediators (SPMs) for combating respiratory health decline in moderate-to-severe COPD patients. Furthermore, our study illuminates DHA as a potential target for therapeutic intervention in promoting respiratory protection. Higher plasma omega-3 levels were associated with better respiratory-specific quality of life and reduced moderate exacerbation risk. It is noteworthy that a 1 SD higher EPA/DHA was associated with a 2.7 lower score in SGRQ, a difference that approaches but does not reach the minimum clinically important difference for the SGRQ, which is generally regarded as 4 points.36 However, many clinical trials of approved medications for COPD37,38 similarly show a ~2.7 difference in SGRQ score. In addition, a larger increase in omega-3 (EPA / DHA), such as 32.9µg/mL or higher, may be required to have a clinically significant change in SGRQ (>4 points). In our cohort, such a large difference in omega-3 is shown when comparing the participants, for example, with the 10>th and 90th percentile levels of omega-3; the bottom 10% of our sample had plasma EPA+DHA levels below 34.9μg/mL while the top 10% were at or above 88.9μg/mL, for a difference of 54.5μg/mL, which would be commensurate with ~6.6 point difference in predicted SGRQ scores.
Omega-3 fatty acids may play a role in airway inflammation of COPD. SPMs, which encompass resolvins, protectins, and maresins, are biosynthesized from EPA and DHA fatty acids and have been shown to regulate and promote the resolution of deleterious inflammation.8 SPMs' homeostatic promotive actions are the result of their stimulation of macrophage phagocytosis of apoptotic cells, cellular debris, and microbes, cessation of superfluous neutrophils (PMN) infiltration, and counter-regulation of pro-inflammatory chemokines and cytokines.39 Maresin-1 (MaR1), a member of the SPM family derived from polyunsaturated fatty acids, specifically DHA, stands out for its potent anti-inflammatory properties in the airway.40 MaR1 exerts inhibitory effects on specific isoforms of protein kinase C (PKC), such as PKCα and PKCε, which are crucial components of the signaling cascade leading to the release of proinflammatory cytokines like TNF-α, IL-6, and IL-8, thereby, effectively reducing their activation.41 Additionally, MaR1 actively promotes the transition of macrophages from the proinflammatory M1 phenotype to the anti-inflammatory M2 phenotype, furthering SPMs’ multifaceted role in resolving inflammation.40 In support of a potentially anti-inflammatory mechanism of action, omega-3 intake, particularly DHA, was associated with lower IL-6 levels in the current study.
As noted, significant associations were found primarily for DHA, and to a lesser extent DPA, when analyzing fatty acids separately. These findings are similar to those found in the study by Patchen et al, which also showed that plasma DHA was associated with attenuation of lung function decline and reduced incidence of airway obstruction.17 Evidence suggests that DHA may signal a reduction in the speed of EPA's metabolic processes, modifying its entry into its metabolic pathway and thereby, potentially reducing the production of downstream anti-inflammatory SPMs.42 However, these DHA and EPA competitive mechanisms, inhibitive processes, and associated effects have yet to be well understood but may explain DHA's potent respiratory protective effects compared to EPA.
While our study provided valuable insights into the relationship between plasma omega-3 levels and COPD morbidity, our study had several notable limitations. Given the seasonal and individual variability in COPD exacerbations, a more extended follow-up period, ideally 12 months or longer, would have been ideal to account for these variables. The sample size was relatively small; however, the longitudinal design (multiple visits per participant) allowed a more robust examination of the associations and gained power. Still, the power was inadequate for several outcomes, including severe exacerbation risk. It is possible that we would have identified additional statistically significant associations with a larger sample size. Our results highlight the need for more extensive studies to fully understand the potential link between omega-3 fatty acids and COPD morbidity. The study did not collect information on whether participants were taking supplementation for omega-3. Hence, the potentially differing role of natural diet versus supplementation on plasma omega-3-COPD morbidity relationship could not be examined. Also, residual confounding could not be ruled out as this study was observational; however, in an attempt to rule out the confounding issue as much as possible, this study included several demographic and COPD-related risk factors, including the indicators of individual and neighborhood socioeconomic status, smoking pack years, BMI, comorbidities, and spirometry-measured lung function at baseline. Still, there are other possible confounding variables, such as whether high omega-3 levels reflect better health care or patient adherence, and unmeasured confounders make it challenging to assign causality and point to a need for randomized controlled trials to better elucidate causal relationships. Previously conducted studies in the United States, which assessed participants' plasma EPA+DHA, reported mean values (55.6–60.8µg/mL)9,43 that were in alignment with our study's sample population (54.02µg/mL). However, it is essential to acknowledge that our study's findings may have limited generalizability for individuals with moderate-to-severe COPD who are current smokers or have higher incomes.
In conclusion, our findings suggest that higher plasma EPA, DHA, and DPA levels in isolation are associated with better respiratory-specific quality of life and lower odds of moderate exacerbations in former smokers with moderate-to-severe COPD. These findings underscore the potential therapeutic benefits of a diet rich in omega-3 fatty acids and lay the groundwork for future prospective clinical trials to investigate the efficacy of such dietary interventions in managing COPD-related morbidities.
Acknowledgements
Author contributions: HW and NNH were responsible for the concept, design, analysis, and interpretation of data. TAK and NNH were responsible for drafting the manuscript. All authors contributed to data analysis, drafting, revision, and final approval of the version submitted for publication and agree to be accountable for all aspects of the work.
Declaration of Interests
NNH reports research grants from the National Institutes of Health’s (NIH) National Institute on Minority Health and Health Disparities related to this manuscript. NNH reports grant support from the Environmental Protection Agency. ALK reports grant support from the NIH during the conduct of the study. TAK, HW, DB, AF, WL, MNE, NP, MCM, EPB, and CH have no financial relationships or conflicts of interest related to the submitted work.