Running Head: Design of the SOURCE Cohort
Funding Support: SOURCE is supported by a National Institutes of Health’s NHLBI grant, R01 HL144718, supplemented by contributions made through the COPD Foundation from Amgen; AstraZeneca/MedImmune; Bayer; Bellerophon Therapeutics; Boehringer-Ingelheim Pharmaceuticals, Inc.; Chiesi Farmaceutici S.p.A.; Forest Research Institute, Inc.; Genentech; GlaxoSmithKline; Grifols Therapeutics, Inc.; Ikaria, Inc.; MGC Diagnostics; Novartis Pharmaceuticals Corporation; Nycomed GmbH; Polarean; ProterixBio; Regeneron Pharmaceuticals, Inc.; Sanofi; Sunovion; Takeda Pharmaceutical Company; Theravance Biopharma; and Mylan/Viatris.
Date of Acceptance: July 30, 2024 | Publication Online Date: August 15, 2024
Abbreviations: BAL=bronchoalveolar lavage; BEACON=British Early COPD Network Cohort; BMI=body mass index; CAAT=Chronic Airway Assessment Test; CanCOLD=Canadian Cohort Obstructive Lung Disease; CAPTURE=COPD Assessment in Primary care To identify Undiagnosed Respiratory disease and Exacerbation risk study; CDART=Carolina Data Acquisition and Reporting Tool; COPD=chronic obstructive pulmonary disease; COPDGene=COPD Genetic Epidemiology study; CSCC=Collaborative Studies Coordinating Center; CT=computed tomography; EBC=exhaled breath condensate; FEV1=forced expiratory volume in 1 second; FTP=file transfer protocol; FVC=forced vital capacity; GINA=Global Initiative for Asthma; GLI=Global Lung Function Initiative; GOLD=Global initiative for chronic Obstructive Lung Disease; HRCT=high-resolution computed tomography; IL-17=interleukin-17; IRB=institutional review board; IT=information technology; LHS=Lung Health Study; MUC5AC=mucin 5AC; MUC5B=mucin 5B; NHLBI=National Heart, Lung and Blood Institute; OSMB=Observational Study Monitoring Board; PRISm=preserved ratio-impaired spirometry; PRM=parametric response mapping; PRMEmph=emphysema as a percentage of total lung vcoxels, determined PRM; PRMfSAD=functional small airways disease as a percentage of total lung voxels, by PRM; SAA=small airway abnormality; SDOH=social determinants of health; SEC/MALS/dRI=size exclusion chromatography with multi-angle light scattering analysis and differential refractive index detection; SOURCE=SPIROMICS Study of Early COPD Progression; SPIROMICS=Subpopulations and Intermediate Outcome Measures in COPD Study; TEPS=tobacco exposure and preserved spirometry; TR=trajectory; UNC=University of North Carolina at Chapel Hill
Citation: Curtis JL, Bateman LA, Murray S, et al. Design of the SPIROMICS study of early COPD progression: SOURCE study. Chronic Obstr Pulm Dis. 2024; 11(5): 444-459. doi: http://doi.org/10.15326/jcopdf.2023.0490
Online Supplemental Material: Read Online Supplemental Material (49,338KB)
Introduction
Chronic obstructive pulmonary disease (COPD) is a highly prevalent, heterogeneous disorder with rising morbidity and mortality.1 Available COPD pharmacotherapy neither reliably alters lung function decline nor prolongs survival,2-4 necessitating radically new therapies. The insights on early disease mechanisms required to develop such therapies cannot come from existing COPD cohorts (including: the COPD Genetic Epidemiology [COPDGene®] study,5 the SubPopulations and InteRmediate Outcome Measures In COPD Study [SPIROMICS],6 or the Canadian Cohort Obstructive Lung Disease7); despite eligibility in those studies at younger ages (Figure 1),8 the mean age at enrollment of their Global initiative for chronic Obstructive Lung Disease1 (GOLD) 0 participants was ~60 years, and very few participants entered before age 55 years. Thus, it is essential to investigate younger individuals at-risk for or with documented features of COPD, focusing on discovering reliable biomarkers of early progressive disease.9,10 To guide such future studies, we led an international group that proposed a working definition for research on early changes leading to COPD (“early COPD”).11

Based on those principles, we designed the SPIROMICS Study of Early COPD Progression (SOURCE), described here, which is funded primarily by the National Institutes of Health’s National Heart, Lung and Blood Institute (NHLBI). The goal of SOURCE is to define the clinical characteristics and biological underpinnings of COPD in younger individuals.9,11 While acknowledging the role of other inhalational exposures in driving worldwide COPD prevalence,12 SOURCE focuses on direct tobacco smoke inhalation (the principal cause of COPD in industrialized nations), to have a single etiological exposure. Enrollment criteria were informed by both pathological13,14 and epidemiological data.15-20 Central to our design were data suggesting that spirometric abnormalities in at-risk individuals were noted by age 43 and that symptoms at ages 36 and 43 predicted subsequent spirometrically-confirmed COPD at age 60–64, whereas symptoms at an earlier age did not.19 The importance of this critical age period has also been recently highlighted by analyses of the Tasmanian Longitudinal Health Study.21 Collectively, these previous studies suggest that airway-centered changes, termed small airway abnormality (SAA), are both an early smoking-induced pathology22 and can lead directly to subsequent emphysema.23,24
Importantly, lung pathology can be identified, COPD heterogeneity characterized, and disease progression predicted and quantified using high-resolution computed tomography (HRCT). Via the analytical technique of parametric response mapping (PRM),25-27 HRCT performed at inhalation and exhalation can distinguish emphysema from nonemphysematous air-trapping due to SAA. HRCT can additionally divide those with COPD into clusters with differing disease progression,28 and can identify the following quantifiable imaging abnormalities associated with accelerated deterioration of lung function: airway wall thickening,29 lower total airway count,30 and airway-to-lung ratio31 (often called “dysanapsis,” a term originally based solely on analysis of maximal expiratory flows,32 but now believed at least partially assessable by imaging33). HRCT imaging can also detect airway mucus plugs, which are associated with multiple adverse outcomes.34-36 Further, more rapid lung function decline in middle-aged individuals is associated with visually-assessed emphysema of moderate or greater severity37 and with >10% low attenuation area.38,39 Accordingly, the SOURCE cohort is powered to detect an imaging-based primary outcome. This approach allows for a smaller sample size than would be the case using spirometric outcomes, which are inherently more variable.
Methods and Materials
The full protocol of the SOURCE cohort is available in Appendix A of the online supplement.
Objectives and Specific Hypotheses
Aim 1 is to determine the relationship in early COPD between initial HRCT-defined SAA and imaging evidence of disease progression. Our primary outcome is a 3-year change in emphysema, as a percentage of total lung voxels determined by PRM (PRMEmph) (Table 1). We postulate that such progression will occur, and that it will correlate with baseline determination of functional small airways disease by PRM (PRMfSAD), in 2 groups of young ever-smokers: those with mild airflow obstruction (GOLD1 stages 1 and 2) and individuals with tobacco exposure and preserved spirometry (TEPS) who have significant respiratory symptoms, determined by a Chronic Airway Assessment Test (CAAT)40 score ≥10. Among older participants in SPIROMICS, we identified symptomatic TEPS as a persistent condition characterized by activity limitation and respiratory exacerbations,41,42 although without airflow obstruction consistent with current COPD diagnostic criteria.
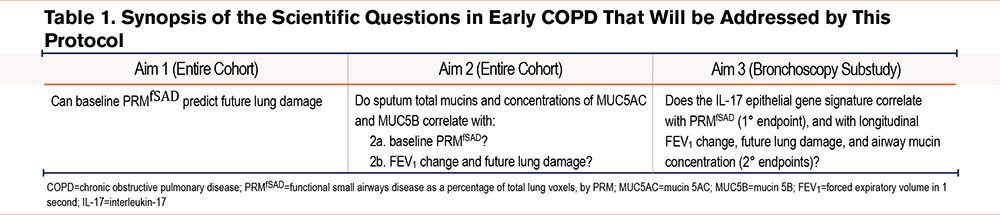
Aim 2 is to determine whether sputum can serve as a less-invasive biomarker of early COPD. We postulate that hyperconcentration of airway mucins, identifiable in specimens collected by sputum induction, contributes centrally both to the development of airflow obstruction and to SAA43-49 (Table 1).
Aim 3 is to define the biological basis of SAA in early COPD. We postulate that SAA is driven by airway inflammation,11 particularly related to interleukin-17-driven inflammation.50,51 We will test this hypothesis via multiple lung-derived biospecimens collected during bronchoscopy (Tables 1 and 2).
Study Design and Organization
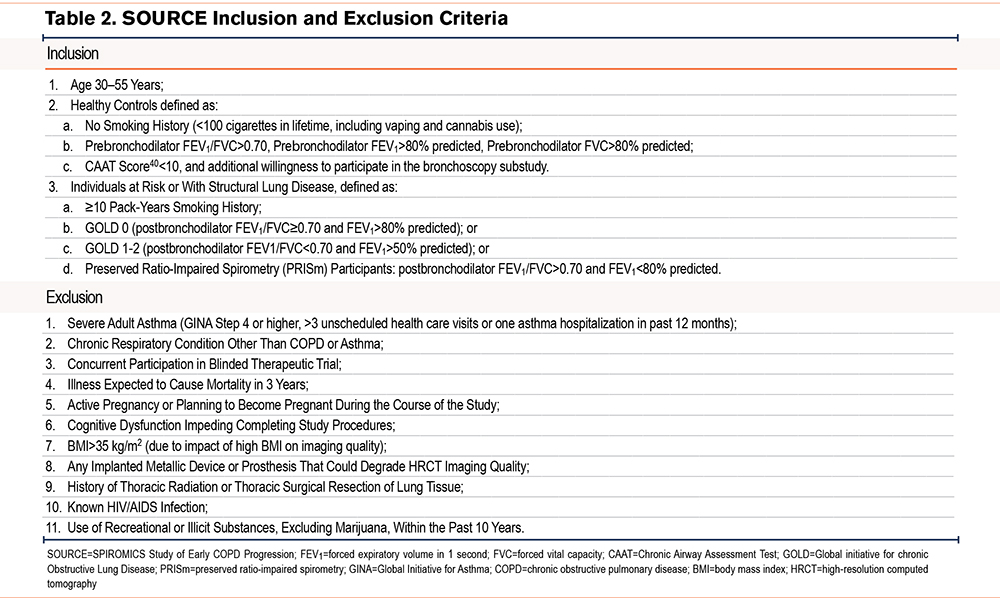
SOURCE is an ongoing (first participant enrolled October 8, 2021) observational cohort study (ClinicalTrials.gov Identifier: NCT05033990), involving 2 study visits, 3 years apart. The cohort is designed to comprise individuals (n=649) 30–55 years old at enrollment, of both sexes, and all races/ethnic backgrounds, with ≥10 pack-years smoking history. An identical study visit will be performed on additional (n=40) never-smokers in the same age range, half of whom must consent to participate in the bronchoscopy substudy, described below. As of April 22, 2024, a total of n=689 participants have been enrolled, with a median age of 48.0 (interquartile range 38.0, 58.0) years.
SOURCE is not a population-based study, but to attempt to minimize bias, neither does it direct recruitment efforts to primary care or specialty clinics, electronic medical records, smoking cessation programs, or other institutional venues designed to enrich for those with respiratory symptoms. Instead, recruitment relies on a strategy described below in “recruitment and retention.” SOURCE is conducted according to the principles of the Declaration of Helsinki; all participants sign written informed consents. Clinical outcomes, including deaths, will be adjudicated centrally.
SOURCE is recruiting participants at 14 clinical centers utilizing the infrastructure of SPIROMICS,6 another ongoing NHLBI-funded observational study designed to identify biomarkers, heterogeneity, and intermediate endpoints of established COPD. Many aspects of data collection are identical, and are also closely related to those of 2 other cohort studies: (1) the British Early COPD Network Cohort (BEACON)52 which between February 2018 and February 2020 enrolled 30–45 year-old individuals (n=431 current tobacco users and 67 never-smokers); and (2) the ongoing Lung Health Study (LHS),53 in which, via NHLBI funding, the American Lung Association is enrolling (n=4000) healthy individuals ages 25–35. Such congruence will permit data from all these cohorts to be combined, enabling future analyses across the entire adult age range of individuals with or at risk of COPD.
Funding is provided by the NHLBI (R01HL144718) and the COPD Foundation, which are involved in study oversight. The protocol has been approved by a single institutional review board (IRB) at the University of North Carolina at Chapel Hill (UNC) and at all clinical sites. An observational studies monitoring board (OSMB) provides semi-annual and ad hoc evaluations with recommendations to the NHLBI. The OSMB monitors the informed consent document and any modifications, data on adverse events (whether anticipated or not), participant safety, progress in enrollment, and on the quality and completeness of study data. The OSMB also reviews ancillary studies to assess possible increase in participant burden. Additional details on OSMB responsibilities are described in the online supplement.
Additional involved agencies are the Collaborative Studies Coordinating Center (CSCC) (UNC), which functions as the data management, clinical, and statistical coordinating center, and biospecimen repository core; an Imaging Reading Center (University of Iowa), a Pulmonary Function Testing Reading Center (University of California, Los Angeles); a Sputum Slide Reading Center (UNC); a Sequencing Center (Weill Cornell); and Immunophenotyping and Microbiome Cores (University of Michigan). Further details about the responsibilities and procedures of these cores is provided in Appendices B-E in the online supplement.
Inclusion and Exclusion Criteria
Before scheduling the in-person visit, via a Health Insurance Portability and Accountability Act waiver, clinical site coordinators contact participants by phone or email to conduct an initial screening questionnaire assessing potential eligibility.
Inclusion criteria for ever-smoker participants align with those proposed to investigate COPD in younger participants10,11 (Table 2). We assess self-reported smoking status at baseline, at the 3-year follow-up visit, and at bronchoscopy, if applicable. Exclusion criteria are designed for participant safety and to minimize confounding causes of lung function decline, interference with the imaging endpoint, or loss to follow-up10,11(Table 2). Individuals with documented immunosuppression, including people living with HIV (even if treated) were excluded based on the postulated central role of lung immunity and inflammation in COPD pathogenesis. Note that a history of asthma or respiratory medication use only during childhood (<18 years old) are not exclusions for the ever-smoker group, but they are for never-smoker control participants, who must also be free of known respiratory disease or symptoms.40 A history of respiratory symptoms compatible with an exacerbation (either solely participant-identified or treated clinically with acute antibiotics or steroids) within the last 30 days is a temporary exclusion, but they can be rescreened for the study ≥30 days after discontinuation of drug therapy.
Power Analysis
The primary analysis will use linear mixed effects models to estimate and perform inference on trajectories of PRMEmph, based on PRMfSAD and PRMEmph at baseline. The power analyses are based on simulations in SAS using Proc Power that assume variability in effect sizes, on a subset of SPIROMICS I participants, age <55 years, GOLD1 stage 0–2, who had imaging data at baseline and at 3 years. Results suggested that for every 10% higher baseline PRMfSAD, there will be ~1% added increase in PRMEmph at 3 years. The simulated power to detect this increase in PRMEmph attributed to baseline PRMfSAD additionally adjusts for baseline PRMEmph. Assuming a Type 1 error of 5% and loss to follow-up of 10%, the simulations indicate >99% power to detect a 1% further increase in emphysema for every 10% higher PRMfSAD at baseline; this result is well within the range of data seen in our preliminary data.
Recruitment and Retention
As a cohort analyzing a disease-state and not a genuine epidemiological cohort, SOURCE was not authorized by NHLBI to employ measures to obtain a truly random, population-based sample. Moreover, the study was designed to maximize recruitment and retention of younger individuals, many of whom are employed or caring for children or elderly relatives. Hence, we have focused self-referral via public-facing social media, rather than on print, radio, or television ads. This approach was informed by the previous experience of our investigative team in recruiting a similar population to the Redefining Therapy in Early COPD Study.54,55
We initially developed a central SOURCE website,56 which included a map of our clinical sites (Figure 2) linking to webpages hosted by them. Besides the hope that brand recognition of those major regional medical centers would enhance participant trust, this process allows immediate capture by the sites of contact and screening information. Study coordinators then rapidly follow up by email, text, or telephone per the preference of interested individuals (at least 5 days weekly, in many cases including in the evening if initial calls during working hours failed).
To direct potential participants to those websites, we developed an intensive social media campaign designed by a company that specializes in recruitment of tobacco users for clinical research studies (BUMP Digital Marketing, Toronto, Ontario). We specifically target the desired age range within geographic extents tailored to each clinical center. The collaboration with BUMP has been essential to recover from delayed enrollment due to the SARS-CoV2 pandemic, which coincided with the funding of SOURCE in May 2020. Moreover, their expertise allowed our campaign to evolve with changes in the privacy policy of major social media platforms that essentially precluded targeting of those who use tobacco products. Although this intensive social media approach necessarily is limited to those with some computer literacy, efforts were made to avoid biasing towards higher levels of education, social class, or health literacy.
Retention strategies include continued engagement via phone call, text message, and/or email every 6 months. IRB-approved newsletters are being sent roughly annually. Participants are compensated for the baseline visit (including a reduced rate for screen-failure) and follow-up visit at 3 years. Bronchoscopy substudy participants receive additional compensation.
Baseline and Follow-Up Assessments
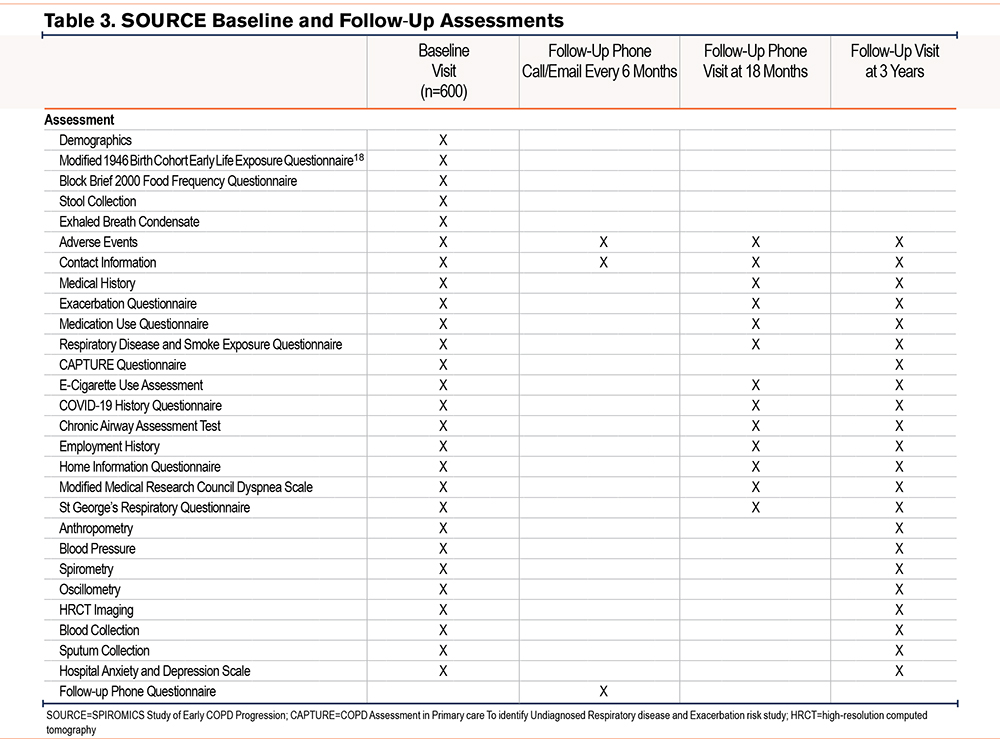
At baseline and follow-up visits, all participants provide detailed information on demographics, exposures, medical history focusing on respiratory symptoms, and medication usage (Table 3). They also undergo biospecimen collection, and the procedures outlined below.
Lung Function Testing
All participants undergo 2 tests of lung function, both pre- and postbronchodilator administration, at baseline and follow-up. The first is respiratory oscillometry, an effort-independent assessment of peripheral, central, or heterogeneous airway abnormalities with reported sensitivity similar or superior to spirometry.57-59 Oscillometry measurements are performed, as described in greater detail in the online supplement, using the Resmon Pro™ (MGC Diagnostics, St. Paul, Minnesota), following technical standards published by the European Respiratory Society.60,61 The second is spirometry, using the Easy One PC spirometer ® (ndd Medical Technologies, Andover, Massachusetts) according to 2019 American Thoracic Society/European Respiratory Society guidelines.62-65 As in SPIROMICS, bronchodilation is induced by 4 puffs each of ipratropium bromide HFA and albuterol sulfate HFA, followed by a 30-minute wait before postbronchodilator testing. The SOURCE protocol was developed using Hankinson predicted values.66 We are aware of recent controversy over use of race- and ethnicity-based adjustments, in which SPIROMICS investigators have taken leading roles.67,68 For consistency during recruitment to the cohort, inclusion criteria were not altered but we have calculated and can make available results using the Global Lung Function Initiative (GLI), “Other,” and “Global” predictions.69 See Appendix B in the online supplement for additional details.
Imaging
Thoracic imaging in SOURCE builds on the extensive experience of the SPIROMICS investigators,70 but uses a novel protocol (developed initially for Precision Intervention for Severe asthma71) designed to minimize radiation exposure in this younger group of participants. At baseline and at the 3-year follow-up, all SOURCE participants undergo 2 series of low-dose lung HRCT scans using iterative reconstruction and dose modulation to adjust for body size on a slice-by-slice basis. Due to dose modulation, radiation dose fluctuates slightly by design between participants of differing builds. Scanners are calibrated using a phantom standard to several U.S. COPD cohorts.72,73 Protocols are specific to scanner make and model, to keep all scanners within comparable levels of noise and image spatial resolution. Hence, target milliampere-seconds and iterative reconstruction parameters differ between participants. We estimate computed tomography (CT) dose index-volume and effective dose for an average-size person with a 30cm scan length. Inspiratory and expiratory scans are performed with breath held at total lung capacity and residual volume, respectively. HRCTs are transmitted to the Imaging Reading Center following a published workflow,70 which includes an automated web portal system.
HRCT generates a very high number of imaging variables, both for whole lung at both total lung capacity and residual volume, and for individual lobes and lung regions. The SPIROMICS investigators have chosen a subset of salient variables considered to be broadly applicable to analyses that use imaging as predictors or outcomes (Supplemental Table 1 in the online supplement). See Appendix C for additional details.
Biological Sample Collection
SOURCE collects a robust set of biospecimens from all participants at both enrollment and at the 3-year follow-up visit (Table 3). To date, the vast majority of participants have agreed to subsequent use by investigators outside SOURCE, including from industry. The SOURCE investigators welcome collaboration and biospecimens can be obtained via approval of an ancillary study.
Blood, Urine, and Nasal Swabs
We collect 7 tubes of blood for future serum, plasma, DNA, and RNA analyses. Additionally, the laboratories at each clinical center perform a complete blood count with differential, capturing variables such as eosinophil counts that are recommended to guide COPD therapy.74,75
Urine is banked for future analyses.76 For participants of childbearing potential, a pregnancy test is performed, and the results received before HRCT imaging.
Because the nasal mucosal transcriptome may reflect pathobiology occurring in the lower respiratory tract,77-82 a nasal swab is collected from the midturbinate region for potential future gene expression studies and microbiome analysis. See Appendix D in the online supplement for details on collection and storage of these sample types.
Exhaled Breath Condensate
Exhaled breath condensate (EBC) is collected only at baseline using the RTube (Respiratory Research, Inc., Austin, Texas), a handheld single-use device. Participants are asked to refrain from eating or drinking for at least one hour before the EBC collection. Consistent with American Thoracic Society/European Respiratory Society recommendations,83 participants wear a nose clip, are cautioned not to touch the chilled sleeve, and are coached to breathe naturally without hyperventilation for approximately 10 minutes, which results in up to 2mL of vapors, aerosols, and moisture collected. Samples will be analyzed as described in the online supplement.
Sputum
See Appendix E in the online supplement for details on sputum induction and sample collection and storage. Briefly, after tongue scraping and gargling in the seated position and without eating for ≥1 hour, participants undergo sputum induction using 0.9%–5% saline (depending on baseline forced expiratory volume in 1 second [FEV1]) via an ultrasonic nebulizer. We monitor drop in FEV1 and use the “whole sputum” method, defined as the raw, unaltered, total expectorated secretions collected. Following removal of raw sample for subsequent mucin and microbiome analysis, at least 75mg of total nonsaliva sputum material must be available for cell-free supernatant recovery and cytospin generation. Cytospins are prepared for differential cell analysis. Supernatant samples are banked for future nucleotide and cytokine analyses, although the absence of protease inhibitors in those samples must be considered. Sputum total mucin concentrations are measured by size exclusion chromatography with multi-angle light scattering analysis and differential refractive index detection (SEC/MALS/dRI) and individual mucin Mucin 5AC and Mucin 5B concentrations are measured by labeled mass spectrometry.84
Stool
Stool samples are banked for future analyses of the gut microbiome as a mediator of respiratory disease. Samples are collected at home using the DNA/RNA Shield Fecal Collection Tube (Zymo Research, Irvine, California), which stabilizes degradation of nucleic acids at room temperature. Participants are given a prepackaged collection kit with barcode label, instruction forms, and mailers permitting return directly to the Microbiome Core via the U.S. Postal Service.
Bronchoscopy Substudy
The bronchoscopy substudy, modeled closely on our previous SPIROMICS substudy,85 will enroll a subgroup of participants at 8 clinical centers. Any ever-smoking participant is eligible (target sample size n=80); agreement to bronchoscopy is an inclusion criterion for never-smokers (n=20). Participants undergo 2 substudy visits. At the first, they are examined by the site bronchoscopist and undergo safety testing (complete blood count, prothrombin/partial thromboplastin time, basic chemistry panel, and pregnancy testing in anyone who could become pregnant). Between 1–12 weeks later, the participant returns for the bronchoscopy procedure.
Details of the SOURCE bronchoscopy substudy will be published elsewhere. Briefly, differences from our published protocol in SPIROMICS I85 include deletion of endobronchial biopsies (not performed in SPIROMICS II or SOURCE), and addition of distal epithelial brushings (performed only at Weill Cornell in SPIROMICS II) at the 7 clinical sites participating in the SOURCE bronchoscopy substudy.86 Epithelial brushes and adherence-purified alveolar macrophages will undergo RNA isolation and sequencing. Using RNA sequence data from the distal and proximal brushes, we will calculate gene signature of type 1, type 2, and type 17 inflammation.51,87 We will establish basal airway cell cultures from distal epithelial brushes, which will be expanded in vitro and cryopreserved for future functional and molecular analyses.86 Specific bronchoscopic brushes will collect airway mucins to compare to sputum results.
From bronchoalveolar lavage (BAL), we will generate cytospin slides for analysis of differential cell counts at the Sputum Slide Reading Center. Viable BAL leukocytes will be analyzed at the Immunophenotyping Core 6 and 24 hours after ex vivo stimulation using agonists recognized by specific host toll-like receptors (TLR4, TLR7/8) to activate innate responses, or by direct T cell activation (anti-CD3 plus anti-CD28). We will reserve supernatants for multiplexed measurement of inflammatory mediators tailored to the cell panel and the stimulus. After staining using panels of phenotypic markers for alveolar macrophages, and subsets of monocytes, dendritic cells, and T cells, and for intracellular production of cytokines (3 per cell type), flow cytometry will be performed and analyzed as described.88,89
Quality Assurance and Control Plan
The CSCC will follow Good Clinical Practice and Quality Guidelines, as standardized and described in the International Council for Harmonisation, for all clinical research study conduct, data management, statistical computing, and biostatistical analysis activities.
To assure data quality and participant privacy, the CSCC follows detailed standard operating procedures. All participant data are entered via electronic case report forms into the Carolina Data Acquisition and Reporting Tool (CDART). This secure, web-based application minimizes the chance of incorrect data entry via extensive cross-checks and automatic calculation of derived variables and total scores from questionnaires. CDART also facilitates completeness of data collection. It has extensive capacity to generate reports with SAS output (including eligibility, windows for follow-up calls, and medication tracking) and to produce mailing labels for sample shipment. Erroneous data entry is minimized via range checks, but when encountered, trigger a protocolized corrective and preventive action process that not only corrects the specific discrepancy but also attempts to prevent recurrence. The corrective action plan is developed and implemented jointly by the data management programmer, software developer, and research staff. Details on the data management plan are provided in the online supplement.
Statistical Analyses
Presentation of results will focus on estimating parameters, such as regression coefficients and correlation coefficients, with corresponding 95% confidence intervals. When reporting p-values, we will give actual values rather than dichotomizing by significance. We will not adjust for data missingness involving few participants (generally <10%), but when the proportion is larger or if potential bias is suspected, we will use multiple imputation by chained equations. Before analyses for a manuscript, additional details, particularly sensitivity analyses and handling of missing data, will be provided in a specific statistical analysis plan.
The primary analysis in Aim 1 will use linear mixed effects models to estimate and perform inference on trajectories of PRMEmph over 3 years, based on baseline PRMfSAD and PRMEmph. In secondary analysis, we will similarly explore the relationship between baseline PRMfSAD and: (1) further increases in PRMfSAD; (2) FEV1 decline over 3 years; (3) changes in oscillometry indices; (4) changes in patient-reported outcomes such as CAAT score40; and (5) respiratory exacerbations.
Aim 1 will also examine the relationship between baseline PRMEmph and further emphysema at 3 years, as supported by preliminary analysis of the subset of participants in SPIROMICS who were in the age range of the SOURCE cohort and who have longitudinal data. Using multivariable linear mixed models, additional analyses will be performed to adjust for age, sex, early life exposures, smoking history, and ongoing smoking status (as a time-dependent covariate where appropriate), baseline FEV1, and concomitant medications. We will perform subgroup analysis of the possible effects of racial and ethnic groups,67 along with status of social determinants of health (SDOH). We will also investigate potential interactions between any of these variables and PRM metrics with the primary outcome, to detect whether any modify relationships between PRM metrics and emphysema development.
The primary analysis of Aim 2 will investigate associations between baseline total sputum mucin concentrations and baseline PRMfSAD. We will perform further analyses using multivariable models to adjust for age, sex, racial/ethnic groups, early life exposures, smoking history and smoking status, concomitant medications, and baseline FEV1% predicted. Potential interactions/effect modification will be explored. We will next investigate the association between baseline mucin concentration and 3-year change in mucin concentrations with progression of PRM-defined HRCT abnormalities and change in FEV1.
Aim 3 is an exploratory analysis designed to generate hypotheses and to provide biospecimens for future ancillary studies. We will correlate baseline PRMfSAD with the interleukin-17 gene signature in airway epithelium51 in both segmental and more distal airways. Secondary analyses will explore correlations of baseline PRMfSAD with: (1) genomic signatures of type 1 and type 2 airway inflammation, (2) functional capacity of ex vivo BAL leukocytes following in vitro stimulation in bulk cultures, and (3) total airway mucin concentration, directly measured from bronchoscopically-collected samples. We will also examine the association of gene expression in the upper (nasal) and lower airways.
Discussion
The SOURCE study is designed with 3 goals: (1) to test whether an imaging biomarker, PRMfSAD, can identify which younger individuals with a smoking history are at-risk for accelerated SAA and hence, early emphysema; (2) to determine whether sputum mucin analyses can noninvasively detect such individuals; and (3) to provide lung-derived biospecimens for mechanistic studies of airway inflammation in early COPD. This cohort will also provide a multitude of biospecimens available for future multiomics analysis (including respiratory and gut microbiome) and correlation with the dense array of physiological, imaging, and exposure data.
Several innovative features of the SOURCE cohort merit mention. Chief, relative to previous large COPD cohorts, is the exclusive recruitment of younger individuals, many without airflow obstruction at enrollment. Due to the high congruence of the SOURCE and SPIROMICS protocols, we can leverage data from those within the appropriate age range when enrolled in SPIROMICS, and extend them by combination with the even younger BEACON and LHS cohorts. Like SPIROMICS, SOURCE focuses on SDOH.67,90 We are aided by the evolution of CT scanners, with improved spatial resolution at significantly lower radiation dose, while still attaining equivalent or improved quantitative measures.70,91-94 This sensitive imaged-based approach enhances the power to identify significant pathways in our biospecimen assessments involving blood, exhaled breath condensate, sputum, and bronchoscopy samples. We will also be able to compare imaging results to noninvasive measurement of small airway function by respiratory oscillometry. The principal limitation of SOURCE is that it is not population-based.
Acknowledgments
Author contributions: JLC takes responsibility for the overall content as guarantor. The manuscript was written primarily by JLC and LAB, based on the study protocol (unpublished). FJM, MKH, and JLC, as cochairs of the SOURCE Executive Committee, led development of the study protocol. All authors engaged in planning various aspects of the study and all authors reviewed the manuscript, provided feedback, and approved the final version.
Data sharing statement: Individual, de-identified participant data from SOURCE, including data dictionaries, will be shared per NHLBI data-sharing policies. Accordingly, databases will be posted to dbGap (https://www.ncbi.nlm.nih.gov/gap/) annually, and will also be available within 6 months of data cleaning via approved ancillary study or manuscript proposals. Details on applying for the latter are posted on the SOURCE website (https://spiromics.org/spiromics/). Additional related documents, including study protocols and statistical analysis plans, will be made available by the same process.
Other acknowledgments: The authors thank the SOURCE participants and participating physicians, investigators, study coordinators, and staff for making this research possible. More information about the study is available at www.sourcestudy.net.
We would like to acknowledge the following investigators of the SOURCE clinical sites and reading centers: Neil E. Alexis, MD; Igor Barjaktarevic, MD, PhD; R. Graham Barr, MD, DrPH; Lori A. Bateman, MS; Richard C. Boucher, MD; Russell P. Bowler, MD, PhD; Stephanie A. Christenson, MD; Alejandro P. Comellas, MD; Christopher B. Cooper, MD, PhD; David J. Couper, PhD; Jeffrey L. Curtis, MD; Mark T. Dransfield, MD; MeiLan K. Han, MD, MS; Nadia N. Hansel, MD, MPH; Eric A. Hoffman, PhD; Yvonne J. Huang, MD; Robert J. Kaner, MD; Mehmet Kesimer, PhD; Jerry A. Krishnan, MD, PhD; Nathanial Marchetti, DO; Fernando J. Martinez, MD, MS; Jill Ohar, MD; Victor E. Ortega, MD, PhD; Robert Paine, III, MD; Stephen P. Peters, MD, PhD; and Prescott G. Woodruff, MD, MPH. The project officers from the Lung Division of the National Heart, Lung, and Blood Institute are Lisa Postow, PhD, and Lisa Viviano, BSN.
Declaration of Interests
JLC reports funding of this project from NIH/NHLBI and the COPD Foundation; grants from NHLBI, NIAID, Department of Veterans Affairs, Department of Defense; consulting fees from CSL Behring, LLC; speaking fees from AstraZeneca; and data safety monitoring board (DSMB) participation for Novartis; all outside this project. LAB reports funding of this project from NIH/NHLBI and the COPD Foundation; speaking fees from Konica Minolta and Continuing Education Alliance, outside this project. SM reports funding of this project from NIH/NHLBI and the COPD Foundation; grants from NIH, outside this project. DJC reports funding of this project from NHLBI and the COPD Foundation. WWL reports funding for participation in this project from K23HL151751 from NHLBI; and personal fees from the Continuing Education Alliance, outside this project. CMF reports funding of this project from NIH/NHLBI and the COPD Foundation; grant support from the Department of Veterans Affairs, and uncompensated service as a board member of the Veterans Education and Research Association of Michigan, outside this project. KBA reports funding for participation in this project from R01HL144849 from NHLBI. SAC reports funding of this project from NIH/NHLBI and the COPD Foundation; grants from NHLBI, American Lung Association; consulting fees from Amgen, AstraZeneca, GSK, Glenmark Pharmaceuticals, and Sanofi/Regeneron; speaking fees from MJH Holdings LLC (Physicians’ Educational Resource, Sanofi/Regeneron, Sunovion, UpToDate, and Wolters Kluwer Health); travel support from AstraZeneca and GSK; DSMB participation for AstraZeneca, GSK, and Sanofi/Regeneron; and an uncompensated board membership for the American Thoracic Company, all outside this project. NEA reports funding of this project from NHLBI and the COPD Foundation. RCB reports grants from NHLBI, NIDDK, the Cystic Fibrosis Foundation, Emergent Ventures, and UNC-Chapel Hill; and royalties, consulting fees, and stock options from Parion Sciences Enterprise Therapeutics, for which he is Board Chairman, all outside this project. RJK reports grants from NHLBI, Boehringer Ingelheim, Bellerophon, CLS Behring, Genentech, Respirvant, Toray and the Department of Defense; royalties from UpToDate; consulting fees from AstraZeneca and Galapagos; speaking fees from Boehringer Ingelheim, the France Foundation, Genentech, and Vindico; DSMB participation for Boehringer Ingelheim, Genetech, Pliant, and PureTech; uncompensated participation in the board of the Pulmonary Wellness Foundation; stock options, for which he paid, in Air Cycle Systems and Doximity; and medical writing fees from AstraZeneca, Boehringer Ingelheim, Galapagos, and Genentech, all outside this project. IB reports grants from Theravance and Viatris and Aerogen; consulting fees from AstraZeneca, Grifols, Inhibrx, Sanofi, Takeda, Theravance and Viatris, and Verona Pharma; speaking fees from Grifols; and membership on the American Thoracic Society Pulmonary Function Committee and the COPD Foundation Nebulizer Consortium, all outside this project. CBC reports funding of this project from NIH/NHLBI and the COPD Foundation; royalties from Cambridge University Press; personal consulting fees from MGC Diagnostics, Chiesi, Herbalide Nutrition Institute, Respiree, and Aer Therapeutics; speaking fees from GlaxoSmithKline and Chulalongkorn University; payment from various law firms; travel fees from MGC Diagnostics; and personal fees for DSMB participation from NUVAIRA and Horizon Therapeutics, all outside this project. EAH reports funding of this project from NIH/NHLBI and the COPD Foundation; and stock options from VIDA Diagnostics, which he founded, outside this project. RGB reports funding of this project from NIH/NHLBI and the COPD Foundation; grants from NIH/NHLBI and the American Lung Association; and membership on the COPD Foundation Medical and Scientific Advisory Committee, outside this project. ERB reports grants from AstraZeneca, Genzyme, Novartis, Regeneron, and Sanofi/Genzyme; consulting fees from AstraZeneca, GSK, Knopp Pharmaceuticals, Novartis, Regeneron, and Sanofi/Genzyme; speaking fees from AstraZeneca; travel support from AstraZeneca, GSK, Novartis, Regeneron, and Sanofi/Genzyme, outside this project. RPB reports funding of this project from NIH/NHLBI and the COPD Foundation; grants from NIH; royalties from Abcam; consulting fees from GNS Health Care, Theravance, and GSK, outside this project. AC reports funding of this project from NIH/NHLBI and the COPD Foundation; grant funding from National Center for Advancing Translational Sciences and the National Institute of Environmental Health Sciences, outside this project; personal consulting fees from GSK, AstraZeneca, Elli Lilly; and nonpaid consultancy from VIDA, outside this project. MTD reports funding of this project from NIH/NHLBI and the COPD Foundation; grants from the American Lung Association and the Department of Defense; Royalties from UpToDate; consulting fees from AstraZeneca, GSK, Novartis, Pulmonx, and Teva; all outside this project. NNH reports funding of this project from NIH/NHLBI and the COPD Foundation; grants from NIH, the COPD Foundation, AstraZeneca, and GSK; DSMB participation for AstraZeneca and GSK, outside this project. JAK reports funding of this project from NIH/NHLBI and the COPD Foundation; grants from NHLBI, the COPD Foundation, American Lung Association, Regeneron, Sergey Brin Family Foundation, and Patient-Centered Outcomes Research Institute; consulting fees from AstraZeneca, BData, Inc., CereVu Medical, GSK and Propeller/ResMed; speakers fees from the American Academy of Asthma, Allergy & Immunology, and the University of Chicago; travel support from the American Thoracic Society and the Global Initiative for Asthma; board membership for the COPD Foundation Medical and Scientific Advisory Committee, the Global Initiative for Asthma, and the Respiratory Health Association, all outside this project. NM reports funding of this project from NIH/NHLBI and the COPD Foundation. DAM reports funding of this project from NIH/NHLBI and the COPD Foundation; grants from GSK; consulting fees from AstraZeneca, outside this project. JO reports a small business grant from NIH; grants from Boehringer-Ingelheim, Sunovion Pharmaceutical, TEVA, Moore Foundation; consulting fees from AstraZeneca, Boehringer-Ingelheim, and Verona; expert testimony fees from Coffey Law, Fox Rothchild, Frankline Casualty, Wallace & Graham, Simmons Hanley, Reid Acree and Kazan Law, all outside this project. WKO reports funding of this project from NHLBI and the COPD Foundation. VEO reports grants from NHLBI; and DSMB submission for Sanofi/Regeneron, outside this project. RP reports funding of this project from NIH/NHLBI and the COPD Foundation; grants from Department of Veterans Affairs; consulting fees from Partner Therapeutics, outside this project. SPP reports funding of this project from NIH/NHLBI and the COPD Foundation; grants from NHLBI; royalties from UpToDate; consulting fees from PPD and Syneos; DSMB participation for GSK and Novartis; all outside this project. JAW reports grants from 37Clnical, AstraZeneca, Boehringer Ingelheim, Chiesi, Genentech, GSK and Novartis; consulting fees from AstraZeneca, Epiendo, Gilead, GSK, Novartis, Pieris, Pulmatrix; speakers fees from AstraZeneca, Boehringer Ingelheim, Novartis, and Recipharm; DSMB participation in Virtus; and board membership on Will March 2022 and the American Thoracic Society, all outside this project. JMW reports funding of this project from NIH/NHLBI and the COPD Foundation; grants from NHBLI, Department of Veterans Affairs, ARCUS-Med, Grifols, Mereo BioPharma, Medscape, and Verona; speaking fees from Medscape; DSMB participation for AstraZeneca, Boehringer-Ingelheim, GSK, and Takeda; stock options from Alveolus Bio; and support for medical writing from GSK and Takeda, all outside this project. PGW reports funding of this project from NIH/NHLBI and the COPD Foundation; grants from NHLBI and Genentech; consulting fees from Amgen, AstraZeneca, Sanofi, and Roche; and speaking honoraria from Hamilton University, Northwestern University and Vanderbilt University, all outside this project. MKH reports funding of this project from NIH/NHLBI and the COPD Foundation; grants from NHLBI, the American Lung Association, AstraZeneca, Boehringer Ingelheim, Biodesix, COPD Foundation, Gala Therapeutics, Novartis, Nuvaira, and Sunovion; royalties from Norton Publishing, Penguin Random House, and UpToDate; consulting fees from Amgen, AstraZeneca, Altesa BioPharma, Aerogen, Boehringer Ingelheim, Devpro, Merck, Mylan, Novartis, Polarian, Pulmonx, Regeneron, Sanofi, Teva, United Therapeutics, and Verona; speaking fees from AstraZeneca, Boehringer Ingelheim, Cipla, Chiesi, GSK, Integrity;DSMB participation for Medtronic and Novartis; board membership for the American Lung Association, the COPD Foundation, American Thoracic Society (journal editor), Emerson School Board, GOLD scientific committee; stock options for Altesa BioPharma and Meissa Vaccines; medical writing for AstraZeneca, Boehringer Ingelheim, GSK and Novartis; and personal fees from Integrity and Medscape; all outside this project. FJM reports funding of this project from NIH/NHLBI and the COPD Foundation; grants from AstraZeneca, Chiesi, GSK and Sanofi/Regeneron; consulting fees from AstraZeneca, Boehringer Ingelheim, Chiesi, CSL Behring, GSK, Novartis, Polaran, Sanofi/Regeneron, Sunovion, Teva, Theravance/Viatris, and UpToDate; speaking fees from AstraZeneca and GSK; DSMB participation for GSK and Medtronic; and remuneration from the American Thoracic Society, all outside this project. MBF and MK report no conflicts.