Running Head: Medicare Advantage Inhaler Education Intervention
Funding Support: None
Date of Acceptance: January 16, 2026 | Published Online Date: February 9, 2026
Abbreviations: COPD=chronic obstructive pulmonary disease; HMO=health maintenance organization; MA=Medicare Advantage; MDI=metered-dose inhaler; pp=percentage points; PPO=preferred provider organization; SD=standard deviation; TTG=teach-to-goal; VBID=value-based insurance design
Citation: Press VG, Katsikas A, Swankoski K, Boudreau E, Thomas E. Phone-based teach-to-goal inhaler education program for Medicare advantage beneficiaries with COPD. Chronic Obstr Pulm Dis. 2026; 13(2): 84-92. doi: http://doi.org/10.15326/jcopdf.2025.0667
Online Supplemental Material: Read Online Supplemental Material (312KB)
Background
Individuals with chronic obstructive pulmonary disease (COPD) often rely on medications to treat and control symptoms delivered through respiratory inhaler devices.1 While the medications are efficacious when delivered to the lung, the majority of patients do not use correct technique,2-11 limiting real-world effectiveness.12 There are numerous types of devices that require different numbers and types of steps, which is further complicated when patients are prescribed more than one inhaler device.10,12-14
To address inhaler misuse, clinical guidelines recommend assessing and teaching inhaler education at all health care encounters.1 However, patients often do not receive inhaler education or receive inadequate instruction due to lack of clinician knowledge, time, or use of ineffective strategies in clinical settings.12,15 Consequences of inhaler misuse and inadequate adherence include decreased symptom control, increased risk of exacerbations, increased acute care utilization, and even death.10-12,16,17 Opportunities to provide education outside of traditional clinical settings could increase delivery of guideline-recommended care and improve outcomes for individuals with COPD.
One innovative approach is to incorporate educational sessions through an insurance-based program. The Centers for Medicare and Medicaid Services offered value-based insurance design (VBID) programs that allowed health plans to offer innovative benefits.18 In 2020, Humana introduced a VBID program for their Medicare Advantage (MA) members with COPD.19 The program was comprised of a medication management program including a phone-based adaptation of the “teach-to-goal” (TTG) inhaler education approach and cost-mitigation through reduced cost sharing for maintenance inhalers.19 The TTG method is an educational strategy to teach correct inhaler technique using the teach-back approach.2,3 The method begins with the patient demonstrating their inhaler use followed by the educator iteratively correcting their technique through rounds of demonstration and verbal instruction paired with the patient’s “teachback” until correct inhaler technique is demonstrated.2,3 The TTG approach has been shown to be more effective in improving inhaler technique compared to less intensive intervention strategies such as a single-set of verbal and written step-by-step instructions.4,5 This is in part due to the “testing effect,”—a cognitive psychology phenomenon whereby memory is enhanced through the act of retrieving information while learning.20 Teachback, the primary technique used in the TTG method, has been endorsed as a patient safety standard by the National Quality Forum for informed consent.21 More recently, teachback is now recommended for inhaler teaching in the COPD clinical guidelines.13,22
In this study we evaluated the effectiveness of the VBID program’s phone-based TTG inhaler education on inhaler technique during the program’s first year.
Study Design and Methods
Overview of the Value-Based Insurance Design Program
Humana’s VBID program was available to all eligible MA beneficiaries with COPD on participating plans, though some beneficiaries were randomly selected for invitation to enroll in the program.19 Beneficiaries were eligible for the program if they had a diagnosis of COPD in the prior 2 years, had filled at least one inhaler prescription (short-acting or maintenance) at least once in the prior year, had a VBID plan, and had low medication adherence (<80%). Patients were excluded from the program if enrolled in the Medicare Part D Low-Income Subsidy program, were in the coverage gap phase of their drug plan, on hospice, had end-stage renal disease, or obtained their primary care at certain Humana subsidiary locations. Patients were included in the program but excluded from analysis when beneficiaries were contractually obligated to be excluded from research, were not continuously enrolled 6 months pre- and 3 months postprogram, and/or if there were missing data. Below, we provide a brief overview of the VBID medication management portion of the program; additional enrollment, randomization, and cost-sharing reduction information is available in Agarwal et al.19
Medication Management Intervention
Enrollees received up to 3 telephone calls from Humana pharmacists for medication management. During the first call, the pharmacist checked eligibility, explained the program, assessed the enrollee’s overall treatment plan and gaps in management, and relayed refill needs to the prescriber including connecting them to a pharmacy if requested. If the enrollee already had access to their inhaler at the time of the initial call, the Humana pharmacist administered TTG education. Otherwise, the Humana pharmacist would schedule a later call to administer the first TTG education session after the enrollee received their inhaler. All enrollees would receive a second TTG education session at least 60 days after their first education session.
Teach-to-Goal Inhaler Education
The TTG education sessions were provided over the phone by Humana-employed pharmacists trained in TTG methodology. An initial “train the trainer” training session occurred in December 2019. The TTG method breaks down the technique for each inhaler into a standardized checklist of 10–17 separate steps, depending on the inhaler (e-Figure 1 in the online supplement). The traditional “in-person” TTG approach was adapted to a phone-based approach for this program to facilitate broad-scale dissemination. Humana’s telephonic adaptation of TTG adhered to the following order of events for each inhaler the beneficiary used: (1) pharmacist assessed the beneficiary’s inhaler technique pre-education by requesting the client verbally report the steps they would take to use the inhaler; (2) pharmacist provided verbal step-by-step inhaler-specific instruction; (3) pharmacist re-assessed the beneficiary’s inhaler technique after the first training by requesting the beneficiary to describe each step of using their inhaler again (post-training 1 assessment); (4) pharmacist provided verbal inhaler instructions again if needed; and (5) if instruction was repeated, the pharmacist conducted another assessment of the beneficiary’s inhaler use by having the beneficiary report the steps they would take to use their inhaler (post-training 2 assessment). All these steps were completed in a single education session (i.e., one phone call). All program participants received 2 education sessions (2 phone calls) (Figure 1).

Data Collection and Outcomes
The TTG pharmacists recorded program participation, inhaler types, assessment scores, and dates in a single documentation tool, RxConsult.23 For each education session we had one pretraining score and the beneficiary’s highest post-training assessment score. We utilized assessment scores to construct the primary and secondary outcomes. Participant’s age, sex, race, dual-eligibility status, eligibility for the Medicare Part D Low-Income Subsidy, primary residence (for classifying participants’ U.S. census geographic region and ZIP-code level population density), and plan type were obtained from Medicare administration data. We constructed comorbidity data using medical claims.
The primary outcome was the difference in the percentage of participants misusing their inhaler(s) before and after the first inhaler education session (session 1 pretraining assessment score minus session 1 post-training assessment score). We classified misuse as conducting less than 75% of steps correctly, as done in prior TTG studies.3-9 “Overall misuse” was evaluated at the member-inhaler level and hence averaged.
A secondary outcome was the difference in the percentage of participants misusing their inhaler(s) before the first inhaler education session and before the second education session. This measure told us the extent to which the inhaler education information was retained between visits. We also calculated the average number of steps conducted correctly.
Regarding enrollee characteristics, we constructed the following demographic variables for each participant: age (categorical: younger than 65, 65–69, 70–74, 75–79, and 80 or older); sex (binary); race (White, Black, other, and unknown); U.S. Census region of the enrollee’s residence (Northeast, Midwest, South, and East); whether the enrollee’s residence ZIP code was in an urban, suburban, or rural area based on Rural-Urban Continuum Codes; the enrollee’s health insurance plan type (health maintenance organization [HMO], preferred provider organization [PPO], or other), and the enrollee’s eligibility for Medicaid or the Medicare Part D Low-Income Subsidy. These characteristics were measured as of the date of the participant’s second assessment. Participants’ clinical characteristics were constructed using medical claims in the 6 months before their first education assessment and measured using the Charlson comorbidity index.
Finally, we obtained COPD Assessment Test data for patients at both educational sessions.
Statistical Analysis
The analysis included 1876 of the 2440 education program participants. Participants were excluded if they were missing education session dates and scores, had nonlogical assessment scores suggestive of assessor error in inputting the data (e.g., scores greater than 100%), or were contractually required to be omitted from research (e-Table 1 in the online supplement). We also required participants to have been continuously enrolled in the medical plan for 6 months before and 3 months after their second assessment to ensure we could measure utilization before and after the program.
We identified the proportion of participants with assessment scores indicating inhaler misuse. We calculated the difference in proportions between assessments and identified statistical significance using 2-way t-tests. Statistical significance was determined by P-values <0.05.
We performed subgroup analyses to estimate whether there were differences in outcomes by age, race (White and non-White), medical plan type (HMO and PPO), and number of comorbidities.
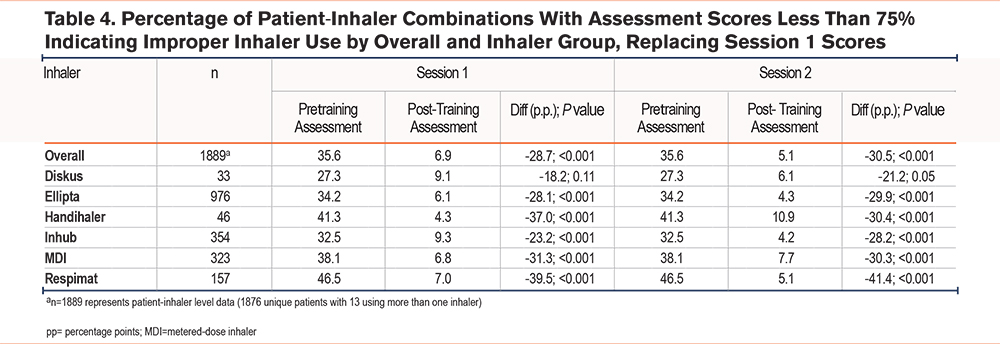
We conducted a sensitivity analysis to address concerns regarding data quality. There was evidence that a data recording issue may have caused a nontrivial proportion of post-training assessment scores to override pretraining assessment scores. The sensitivity analysis replaced the pretraining scores from the first session with the pretraining scores from the second session. Our rationale for this approach is that the pretraining scores from the second session were either similar or better than the true pretraining scores of the first session but likely smaller than the first session’s post-training scores. Prior studies where follow-up assessment occurred showed that significant improvements in technique found immediately after the first educational session were no longer present within a month.4,5
Analyses were performed using SAS Enterprise Guide, version 8.3 (SAS; Cary, North Carolina). This study was granted exemption from an institutional review board review by the Humana Healthcare Research Human Subject Protection Office.
Results
Enrollee Characteristics
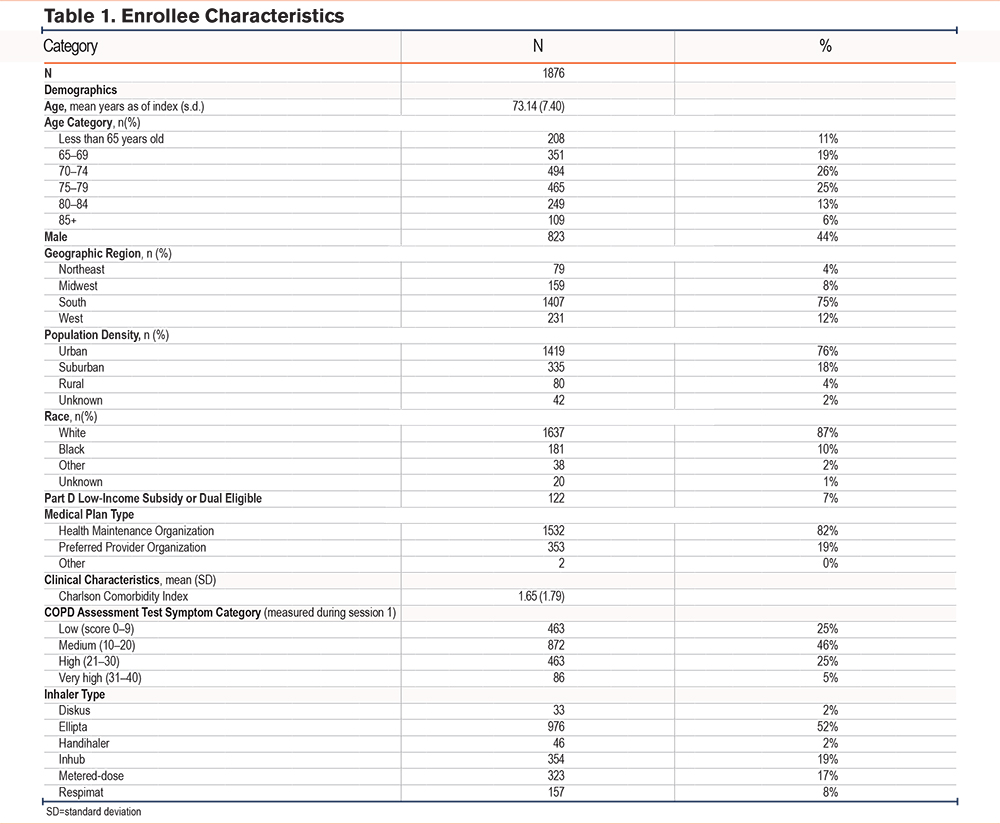
Of 1876 unique participants eligible for inclusion in the analysis between January 1 and December 31, 2020, 68% (n=1276) were targeted for enrollment and received program outreach, while 32% (n=600) self-enrolled in the TTG program. Of 1876 patients analyzed, 13 (<1%) used more than 1 inhaler (n=1889 inhaler evaluations). The mean age was 73 years, most were women (56%), White (87%), living in the South (75%), and in urban (76%) settings. Most participants were in HMO plans (82%). Participants had on average (mean) 1.65 comorbidities, with the most common comorbidities other than COPD being peripheral vascular disease (14%) and renal disease (13%). The most common inhaler type was Ellipta (52%) (Table 1).
Inhaler Technique
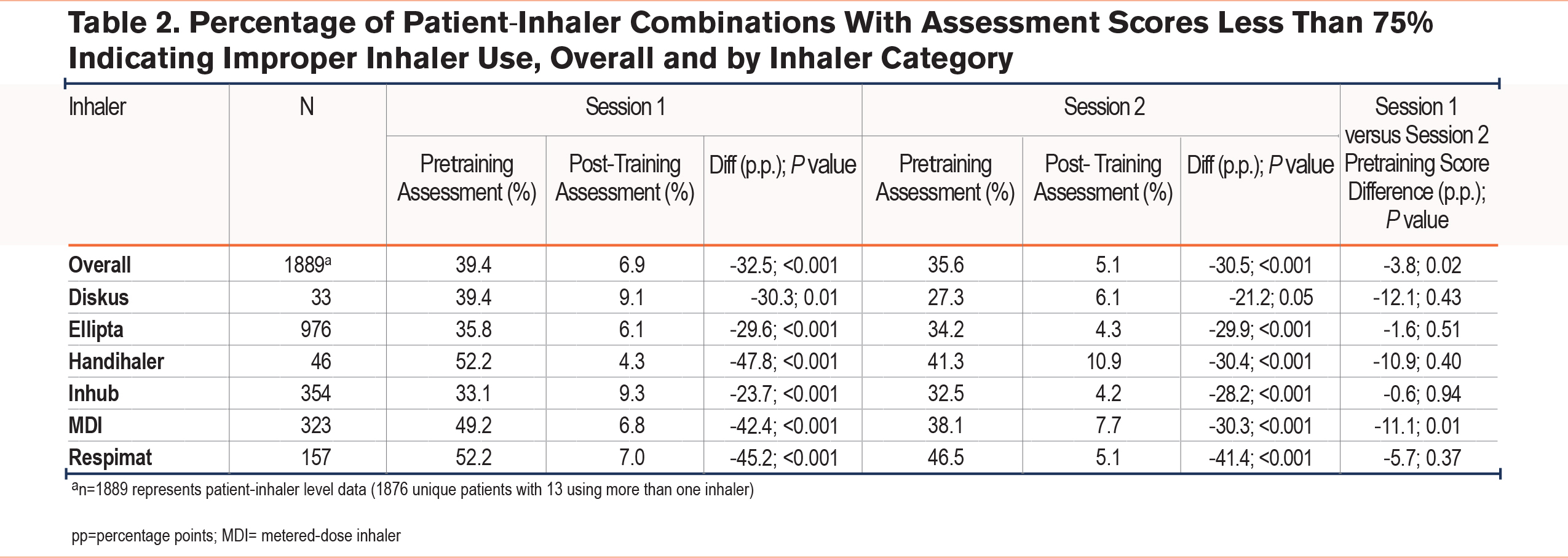
At the initial assessment, 39.4% of participants were using their inhalers incorrectly (Table 2). This varied by inhaler type, with several inhaler device types being misused by about half of participants: MDI (49.2%), Handihaler (52.2%), or Respimat inhalers (52.2%). By the end of the first education session, the percentage of participants who were using their inhaler incorrectly decreased from 39.4% to 6.9%, with the largest improvements occurring among the MDI (6.8%), Handihaler (4.3%), and Respimat inhalers (7.0%) (Table 2).
Comparing the pretraining scores from the first and second education sessions (the 2 sessions were about 60 days apart), there was a moderate decrease in inhaler misuse over time. For example, there was an overall decrease in the percentage of participants misusing their inhaler of about 3.8 percentage points, from 39.4% at the first session to 35.6% at the second session. There were notable reductions in misuse among Handihaler (52.2% to 41.3%), Diskus (39.4% to 27.1%), and MDI (49.2% to 38.1%) inhaler users with reductions of 10 percentage points or more between the first and second session, though only the MDI saw significant differences between the first and second session (Table 2).
Analyses of the average assessment scores showed similar results. The average initial assessment score was 75.7 out of 100, increasing to 90.9 at the end of the first session and 93.1 at the end of the second session (e-Table 2 in the online supplement).
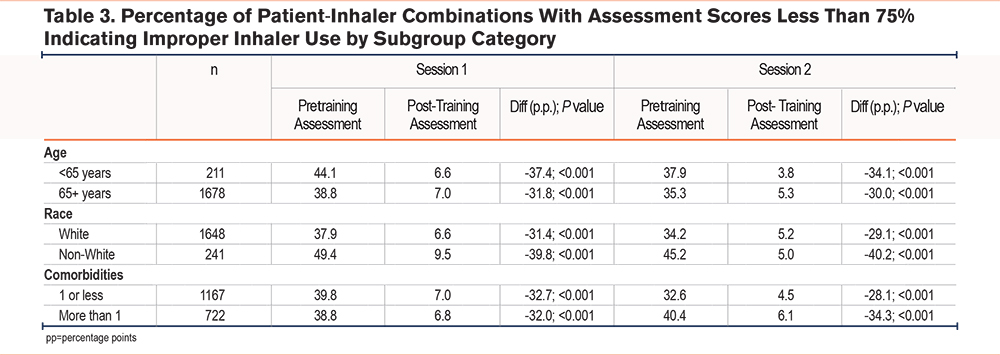
With regard to subgroups, while misuse significantly decreased across all subgroups post-versus pretraining, some subgroups had higher baseline misuse and/or had greater decreases in misuse (Table 3). For instance, inhaler misuse was greater among younger beneficiaries (44.1%) compared to older beneficiaries (38.8%) misused pretraining, but lower post-training (6.6% versus 7.0%, respectively). White beneficiaries had lower inhaler misuse pre- and post-training compared to non-White beneficiaries (37.9% versus 49.4%; 6.6% versus 9.5%). Differences were not seen among those with low or high levels of comorbidities pre- or post-training.
Sensitivity Analysis
Results of the sensitivity analysis were similar to those from the primary analysis (Table 4). After replacing the pretraining assessment scores from session 1 with the pretraining assessment scores from session 2, the percentage of participants misusing their inhalers decreased slightly. The improvement in inhaler use between the pre- and post-scores during session 1 also decreased slightly, as expected, due to the pre-scores at the second session being higher than the initial assessment scores.
Discussion
We found that patients improved their inhaler technique across all inhaler types through the 2-session phone-based TTG inhaler education program. Importantly, the second education session was likely critical for longer term technique since initial improvements in inhaler technique seen after the first education session were not consistently maintained prior to the second session. Additionally, some subgroups had higher levels of baseline inhaler misuse, though all subgroups showed decreased misuse post-education. These findings further support the use of TTG inhaler education which now aligns with more recent COPD guidelines that suggest the use of “teach-back’” as an effective strategy.1,13,22
It is notable that this phone adaptation of a traditionally in-person TTG educational strategy was still effective, despite lack of visualization by the educator or the beneficiary. Without visualization by the educator of the beneficiaries’ baseline or post-training inhaler technique, it is possible that they provided correct actions without being able to conduct the steps correctly. Importantly, a direct-to-patient adaptative learning module called “virtual” TTG that does not have a live educator, but rather the individual uses a learning module to test their knowledge and learn correct technique,6,24 has been shown to be noninferior to in-person TTG.7 Future noninferiority studies are needed to test in-person TTG compared to phone-based TTG to determine whether phone-based TTG is as robust and effective as TTG for improving visualized inhaler technique and clinical outcomes. If phone-based TTG is as effective, this could allow for clinicians, health systems, and health plans to scale this approach to a larger group of individuals with COPD.
With respect to overall levels of misuse, the proportion of patients misusing inhalers decreased significantly between the pretraining and post-training assessments within the first session from one-third to one-half misusing to less than 10% for all inhalers. These results validate previous findings that after a single TTG educational session, inhaler misuse decreases for most individuals.5,8,9 Also notable was the need for a second educational session due to levels of misuse rising again across inhaler types between the first and second sessions. While the precise level of “dosing” or number of educational sessions needed for long-term effectiveness is unknown, even one session has been found to reduce short-term acute care utilization,4,5 and multiple sessions have been found to improve adherence,9,19 quality of life,9 and self-efficacy,9 in addition to inhaler technique.8,9
Importantly, while improvements were seen across devices, not all inhalers had the same degree of effectiveness with TTG. We observed heterogeneous outcomes with Handihaler, MDI, and Respimat inhaler users demonstrating the most significant improvements. These groups experienced nearly 50 percentage point reductions in the proportion of misusers between the post-training and pretraining assessments within the first session, respectively. This contrasts with the Inhub and Ellipta inhaler users that demonstrated smaller, but still meaningful reductions in the first session. This heterogeneity is unsurprising because prior studies have found that some inhalers are more difficult to use and learn to use than others.4,5,10,11,14,17,25,26
Further, not all subgroups had the same baseline level of misuse or, in some cases, equivalent responses to the TTG education. Due to the large study cohort, these findings are novel and may shed light for identifying at risk groups and groups that may benefit more than others from the education. For instance, younger beneficiaries had more baseline misuse but less misuse after TTG compared to the older beneficiaries. Specifically, younger beneficiaries qualified for Medicare due to disability as opposed to being age-based. Further research is needed to learn if adjustments in the inhaler education are needed to accommodate different beneficiaries’ needs.
While more than one educational session is necessary for most individuals, the largest improvements in inhaler use were concentrated in the first TTG session. This is not surprising as some individuals retained the education from the first session dampening the potential effect seen both in this study and in prior studies.5,8,9 However, despite less of an effect, there was still substantial improvement after the second session. It is still not known, however, whether 2 sessions are adequate and what the ideal intervals should be. Future studies are needed to evaluate longer term sustainability of the multisession education and effects on clinical outcomes.
This study had several limitations. First, we cannot draw causal inferences from these results because the TTG education was delivered in combination with the cost-savings component of the VBID program. Likewise, we were unable to identify a valid control group against which to compare changes in inhaler misuse over time. Therefore, we can only infer associative conclusions based on these results. Further, given the pragmatic implementation of this program, real-world data capture was challenging, and complete accuracy was not likely. For instance, there were data capture issues for inhaler technique scores, but an exact number of patients for whom this was an issue was not known. Also, this led to nearly one-quarter of participants whose data were not analyzed. In addition, the program targeted patients with fill-related adherence of less than 80% based on days covered. Therefore, this approach may limit the generalizability of our findings to broader populations, as adherence behaviors in other groups may respond differently to the intervention. Additionally, individuals received the program via 2 different pathways, namely being invited into the VBID program or receiving the TTG training through an independent pathway. Individuals may have responded differently to the program depending on their method of joining the program. Finally, this was a real-world program whereby pharmacists were trained on the phone-based TTG approach but could have altered their educational strategy without being able to observe or measure these adjustments.
Despite these limitations, the effects of this phone-based TTG program are congruent with prior studies of in-person, video-based, and video-module based TTG inhaler education studies,2-9 which all show that use of TTG inhaler education is effective. The results from this study demonstrating the effectiveness of TTG and our prior work demonstrating improved medication adherence19 could have greater implications for supporting additional medication management programs for patients with COPD. This pharmacist-led phone-based education could be readily adapted and disseminated across other payers and/or health care settings.
Conclusion
A phone-based adaptation of a TTG inhaler education program offered by a large national health plan demonstrated improvements in inhaler technique across different types of inhaler devices and among different subpopulations. The multiple session approach was likely critical for longer term retention of correct technique, though further study is needed to confirm this. Some subgroup populations are also at greater risk for baseline inhaler misuse and/or post-training inhaler misuse indicating a need for further evaluation of how to tailor inhaler education by individuals’ needs.
Acknowledgements
Author contributions: VGP takes responsibility for the content of the manuscript. AK, KS, EB, and ET contributed substantially to the study design, data analysis and interpretation, and the writing of the manuscript. All authors approved the final version submitted for publication.
Other acknowledgements: We would like to thank Elizabeth Metzler for her contribution to the program. We would like to thank the pharmacists for their participation in the program.
Declaration of Interest
VGP reports receiving grant funding from the National Institutes of Health and the Agency for Healthcare Research and Quality. She also reports receiving consulting fees for her work with Humana on this educational program. EB reports employment and equity holdings with Humana. All other authors have no conflicts or funding to report.