Running Head: COPD Patient Perspectives, Wildfire Smoke Exposure
Funding Support: Research reported in this publication was supported by the National Heart, Lung and Blood Institute of the National Institutes of Health under Award Number K23HL173649. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Date of Acceptance: March 11, 2026 | Published Online Date: March 30, 2026
Abbreviations: COPD=chronic obstructive pulmonary disease; NDI=neighborhood deprivation index; SD=standard deviation
Citation: Yao J, Lydon CM, Pak N, et al. Understanding COPD patients’ perspectives on utilizing strategies to limit their exposure to wildfire smoke. Chronic Obstr Pulm Dis. 2026; 13(3): 206-215. doi: http://doi.org/10.15326/jcopdf.2025.0682
Online Supplemental Material: Read Online Supplemental Material (599KB)
Introduction
Long-term exposure to wildfire smoke is associated with increased mortality.1 As a direct result of climate change, wildfire smoke is responsible for a growing fraction of particulate matter air pollution in the United States.2 Patients with chronic obstructive pulmonary disease (COPD) are at especially high risk of exacerbation due to wildfire smoke, as up to 30% of exacerbations are due to environmental triggers.3,4 Existing literature supports a dose response relationship with one study reporting a 2.7% increase in COPD exacerbations for every 10µg/m3 rise in particulate matter exposure.5,6 Although people living on the West Coast are considered to be at highest risk of exposure to wildfire smoke, smoke originating on the West Coast travels east with the jet stream, putting the entire country at risk.7,8
The health burden of wildfire smoke falls disproportionately on vulnerable populations, especially those with low socioeconomic status.9-11 This is thought to be due to lower quality housing structures, which allow particles to enter the indoor space through cracks around windows and door frames, and poorly filtered air coming through the heating and ventilation system.12-14 Additionally, vulnerable populations have fewer educational and financial resources to buy protective equipment, including air cleaners, to safeguard themselves during periods of poor air quality.9
In a workshop report, an American Thoracic Society panel identified the following strategies for mitigating wildfire smoke exposure at the individual level: (1) staying indoors, (2) wearing N95-rated respirator masks when outdoors, (3) using vehicle air recirculation settings, (4) periodically replacing the home’s ventilation system filters, (5) sealing windows/doors, and (6) utilizing portable high-efficiency particulate air cleaners.15 These mitigation strategies are recommended by the Environmental Protection Agency and Centers for Disease Control and Prevention.16,17 Despite the ability of indoor air cleaners to reduce indoor particle concentrations by 40%–80% and reduce respiratory symptoms in COPD patients when used over 6 months in an urban setting,18 studies have shown limited uptake of portable air cleaners (and other mitigation strategies).12
In this study, we performed qualitative interviews with patients aged ≥65 years old with COPD and low socioeconomic status, who lived in close geographic proximity to historically large wildfires. The goal was to gain insights from patients to inform the design of intervention(s) that can be deployed to increase uptake of the aforementioned mitigation strategies and protect this vulnerable patient population from the harm of wildfire smoke.
Methods
This study was approved by the Kaiser Permanente Northern California Institutional Review Board (Protocol 2131623-10) with a requirement for verbal consent.
Design and Setting
We conducted qualitative, semistructured interviews, in which we enrolled patients with COPD within Kaiser Permanente Northern California, the largest integrated health system in the United States, serving >4.5 million patients as a health insurer and health care provider. Supplement S1 in the online supplement contains the 32-item checklist for the Consolidated Criteria for Reporting Qualitative Studies.
Developing the Interview Guide
We developed an interview guide at a ≤ 5th grade literacy level with 3 sections: relationship with and understanding of wildfire smoke, use of strategies for protecting one’s health from smoke, and experience with prescribed burns (Supplement S2 in the online supplement). The interview guide was developed by LCM with edits from CML and KAD and expert guidance from AA.
Participant Recruitment
Potentially eligible participants were initially identified using electronic health record data (Supplement S3 in the online supplement). Patients were eligible if they met 3 criteria:
1. Received COPD as an International Classification of Disease-10th edition coded diagnosis (J44.1, J44.0, J41.8, J44.9, J42) between 9/30/2021–10/31/2024 during either at least 1 hospitalization or at least 2 outpatient encounters;
2. Were ≥65 years old;
3. Had an active Kaiser membership as of 10/31/2024.
We further narrowed to those with a neighborhood deprivation index (NDI)19 in the highest quartile in order to focus on those with low socioeconomic status. The diagnosis code definition of COPD produces sensitivity (69.2%) and specificity (93.2%).20 The rationale for recruiting those ≥65 years old was to enrich for patients with COPD (versus asthma), to interview patients with enough lived experience over time with smoke from any source, and to interview patients who would ultimately be the target population of an intervention (patients aged >65 years spend >80% of time at home where you would deliver a home intervention, such as air cleaners).21,22
We excluded patients who could not speak English, were enrolled in hospice, had a tracheostomy, or did not have a mailing address (presumably undomiciled). We emailed patients’ primary care physicians to further identify anyone who should not be contacted for recruitment due to issues not readily identified above.
To stagger enrollment, we proportionally divided the list into 3 equally sized groups with the same distribution of zip codes. The first group received an information packet mailed to their homes. Because recruitment proceeded quickly, saturation was reached before further mailings were needed.
Conducting the Interviews
An internal medicine trained male physician (JY), a Master of Public Health student at the time, conducted the interviews. JY received both formal (UC Berkeley) and informal training (mentorship at Kaiser Permanente Northern California Division of Research) in qualitative methods. Verbal consent was obtained over the phone prior to initiating the interview. Interviews lasted ~30 minutes and were conducted securely via Microsoft Teams, utilizing embedded voice-to-text transcription. Interviews were scheduled until the point of thematic saturation, when repeated themes emerged with each additional interview.23 Field notes were written after each interview by LCM upon listening to the recordings. The output files were deidentified and loaded into standard qualitative interview software (Dedoose 10.0.25; Los Angeles, California). Participants did not provide feedback on the interview transcripts or themes.
Qualitative Analysis
We performed traditional thematic analysis through the iterative process of analyzing patterns in qualitative data. We took both inductive and deductive approaches. Initially, an inductive approach was utilized where themes emerging from participants’ responses were collected into a codebook. The codebook was drafted by JY, modified by CML and LCM using the first 5 interviews, and revised by expert AA (Supplement S4 in the online supplement). The team ensured that the coding structure reflected the lived experiences and perspectives of participants. Once the codebook was agreed upon, JY manually coded the remaining interview transcripts for recurring themes and categories. Meanings were considered primarily at the explicit level but with consideration of implicit interpretations. Illustrative quotes were flagged. To make the findings as practical as possible, we provide examples of practical insights into how an intervention could be designed based on the barriers and facilitators elicited during the interviews.
Results
Description of Participants and Their Relationship With Smoke
Of 90,696 adults aged ≥65 years with COPD, 6338 met all inclusion/exclusion criteria (full details in Supplement S3 in the online supplement). Of the 2112 patients who received the initial recruitment packet in the mail, 180 patients contacted us, of whom 107 stated they were potentially interested. We scheduled interviews between 1/7/2025–1/21/2025 in the order in which people expressed interest.
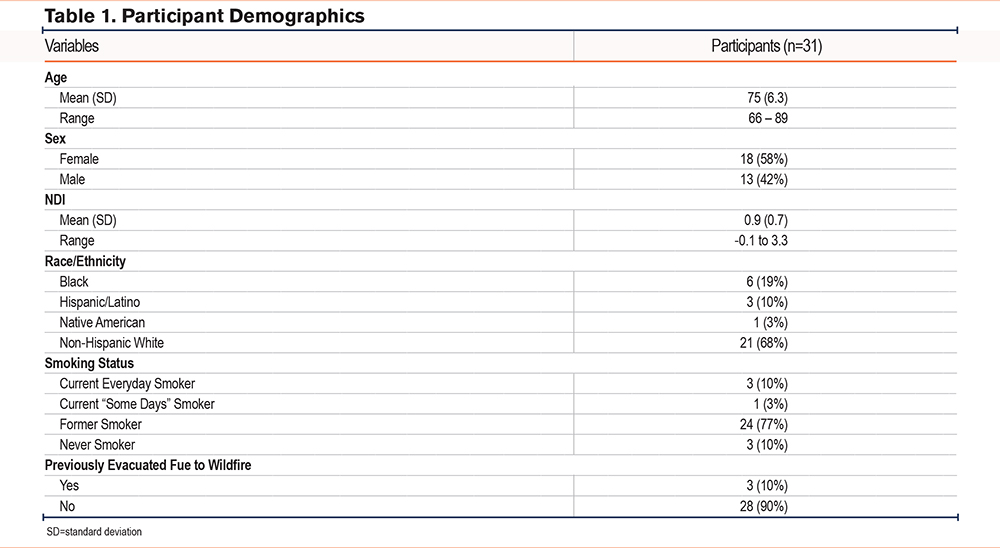
The demographic characteristics of the 31 participants are listed in Table 1. The average age was 75 years old (standard deviation [SD] 6.3). Eighteen participants (58%) were female. Average NDI was 0.9 (SD 0.7). Participant’s self-identified race/ethnicity was 19% Black, 10% Hispanic, 3% Native American, and 68% non-Hispanic White. Individuals lived in 10 counties across Northern California: Alameda, Contra Costa, San Mateo, Sonoma, Stanislaus, Solano, Madera, San Joaquin, Sacramento, and Fresno. Nearly all (n=28, 90%) interviewees had some form of cigarette/cigar smoking history, and 4 (13%) identified as current smokers. Most interviewees (n=28, 90%) denied having to evacuate their homes for a past wildfire. One participant reported working as a firefighter previously.
Participants described neutral or even positive experiences of smoke exposure from fireplaces and campfires but described negative experiences toward cigarette/cigar smoke, wildfires, or structural fires. Most participants stated that they believed their health has been more impacted from repeated exposure to smoke over time, especially cigarette smoke, rather than a 1-time exposure, such as a wildfire. When asked which organ(s) are affected by smoke, few named >1 organ beyond the lungs. They reported feeling more concern about smoke exposure later in life due to instances when smoke has triggered respiratory symptoms (e.g., shortness of breath, chest tightness). Despite concerns about smoke, nearly all of participants stated they supported the use of prescribed burns because the public could be made aware of the smoke ahead of time and such prescribed burns could offset the risk of larger wildfires. Most participants stated that they were not regularly thinking about wildfire smoke (e.g., on a week-to-week basis) unless there was a wildfire event in the news.
Major Themes Elicited
Table 2 depicts the major themes, which are described below with illustrative quotes.
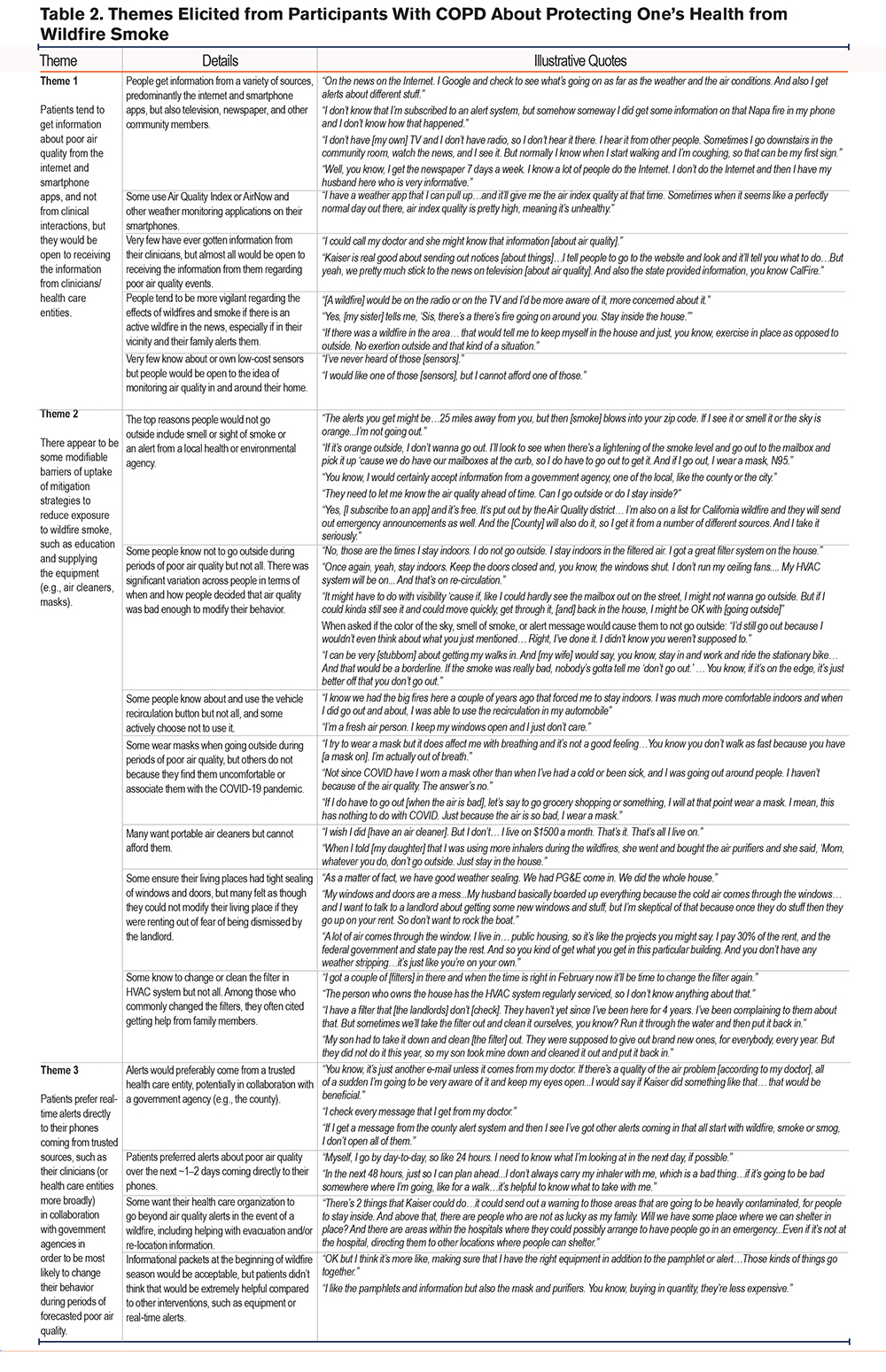
Theme 1
Patients tend to get information about poor air quality from the internet and smartphone apps, and not from clinical interactions, but they would be open to receiving the information from clinicians/health care entities.
People got their information from a variety of sources, predominantly the internet and smartphone apps, but also television, newspaper, and other community members. One participant said they received air quality information from “the news on the Internet. I Google and check to see what's going on as far as the weather and the air conditions.” Another stated, “I don't have [my own] TV and I don't have radio...I hear it from other people. Sometimes I go downstairs inthe community room, watch the news, and I see it.” Some used Air Quality Index or other weather monitoring applications on their smartphones. One participant stated, “I have a weather app…and it'll give me the air index quality at that time. Sometimes when it seems like a perfectly normal day out there, air index quality ispretty high, meaning it's unhealthy.” Very few had ever gotten information from their clinicians, but almost all would be open to receiving the information from them regarding poor air quality events. Additionally, very few knew about or owned low-cost sensors but would be open to the idea of monitoring local air quality in and around their homes.
Theme 2
There appear to be some modifiable barriers of uptake of mitigation strategies to reduce exposure to wildfire smoke, such as education and supplying the equipment (e.g., air cleaners, masks).
The top reasons people would not go outside included smell or sight of smoke or an alert from a local health or environmental agency. One participant described their thought process in terms of deciding whether to go outside, “The alerts you get might be…25 miles away from you, but then [smoke] blows into your zip code. If I see it or smell it or the sky is orange...I'm not going out.”While some people felt confident that they knew when air quality was at a level that was harmful to health, not everyone did. When asked if the color of the sky, smell of smoke, or alert message would cause them to not go outside, one participant admitted, “I'd still go out because I wouldn't even think about what you just mentioned… I've done it. I didn't know you weren't supposed to.” There was significant variation in when and how people decided that air quality was bad enough to modify their behavior.
Many of the barriers of uptake of mitigation strategies were modifiable through education or direct provision of equipment. In terms of knowledge of specific mitigation strategies, some people knew about and used the vehicle recirculation button but not all, and some actively chose not to use it. Someone explained, “I'm a fresh air person. I keep my windows open and I just don't care.” Some wore masks when going outside during periods of poor air quality, but others did not because they found them uncomfortable or associated them with the COVID-19 pandemic. Many expressed interest in and desire for portable air cleaners but cited finances as the main barrier, “I wish I did [have an air cleaner]. But I don't…I live on $1500 a month. That's it. That's all I live on.” Some ensured their living places had tight sealing of windows and doors, but many felt they could not modify their living place if they rented out of fear of being evicted by the landlord. One participant explained, “A lot of air comes through the window. I live in…public housing, it's like the projects you might say… you kind of get what you get in thisparticular building. You don't have any weather stripping…it's just like you're on your own.” Another said, “My windows and doors are a mess...My husband basically boarded up everything because the cold air comes through the windows… I want to talk to a landlord about getting some new windows and stuff, but I'm skeptical of that because once they do stuff then they go up your rent. Don't want to rock the boat.” Lastly, some knew to change or clean the filter in HVAC system but not all. Among those who commonly changed the filters, they often cited getting help from family members.
Theme 3
Patients prefer real-time alerts directly to their phones coming from trusted sources, such as their clinicians (or health care entities more broadly) in collaboration with government agencies, to be most likely to change their behavior during periods of forecasted poor air quality.
Patients overwhelmingly expressed trust in their clinicians or health care entities with one participant saying, “You know, it’s just another e-mail unless it comes from my doctor. If there's a quality of the air problem [according to my doctor],all of asudden I'm going to be very aware of it and keep my eyes open.” Another said, “I check every message that I get from my doctor.” Many expressed similar views, stating that they’d be more likely to modify their behavior if the alert came from a health care entity that knew them and their medical history, potentially in collaboration with a government agency.
When asked about what type of alerts were preferred, participants overwhelmingly endorsed forecasted air quality alerts for the next 1–2 days coming directly to their phones. One endorsed, “In the next 48 hours, just so I can plan ahead...I don't always carry my inhaler with me, which is a bad thing…if it's going to be bad somewhere where I'm going, like for a walk…it’s helpful to know what to take with me.” In addition to alerts about air quality, several mentioned wanting to hear information about emergency evacuation and relocation. One suggested, “There are areas within the hospitals where they could possibly arrange to have people go in an emergency...Even if it's not at the hospital, directing them to other locations where people can shelter.”
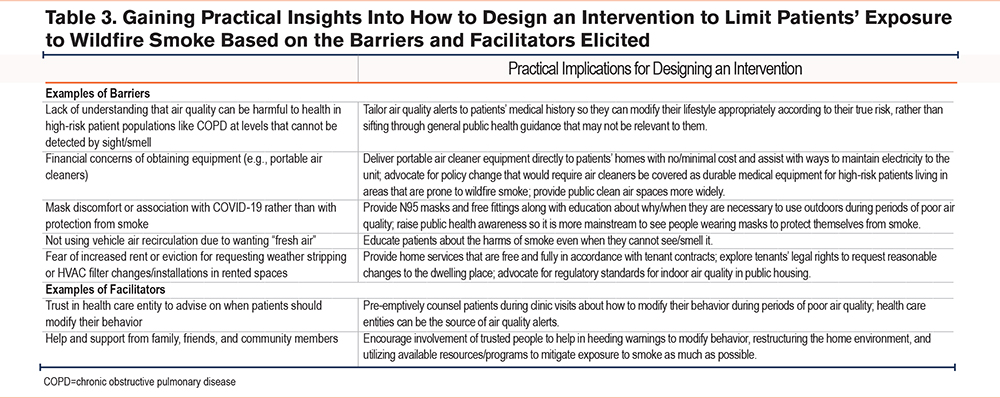
Turning the Barriers and Facilitators into Practical Insights for Designing an Intervention
We provide several examples of how the barriers and facilitators elicited during the qualitative interviews provide practical information for designing future interventions (Table 3). For example, an air quality alert intervention where alerts are tailored to patients’ medical history and come from a trusted health care entity would overcome the barrier of patients not knowing when to modify their behavior and leverage the facilitator of trusting their health care system to advise on their health. Alternatively, a home intervention where education and equipment are brought directly to patients’ homes, potentially with engagement of family members during the home visit, would overcome the barriers of lack of knowledge and financial concerns about obtaining equipment, as well as leverage the help of family to support vulnerable patients during periods of poor air quality.
Discussion
Among COPD patients with low socioeconomic status, we utilized a qualitative approach to understand patients’ perspectives about the ways they protect their health in the setting of poor air quality events, including the barriers and facilitators related to uptake of mitigation strategies that reduce wildfire smoke exposure. While we anticipated hearing about financial barriers to obtain equipment, we uncovered several key insights, such as how rare it was that patients had received information from clinicians about the health risks of smoke, the degree of trust that patients put in health care entities to advise them on when to modify their behavior in relation to smoke, the fear of losing access to rented housing if they were to ask the landlord for weather stripping or air filter changes, and the important role of family/community members to help this vulnerable patient population modify their homes or individual behaviors. Health-promoting behavioral interventions have been shown to be more effective when multidisciplinary community support organizations come together24 (in this case, it would potentially be health system and public health through the county/state).
While there is extensive quantitative research documenting the epidemiologic associations between concentrations of particulate matter air pollution and poor health outcomes,1,5 there is less qualitative information to help guide the design and deployment of interventions, which is the important gap that this study fills. Studies done across the world in settings prone to wildfires have found broad themes similar to us, such as need for education, provision of equipment, and accurate, real-time information.11,25-29 Our study extends the existing qualitative literature about how high-risk patients (older COPD patients with low socioeconomic status) can protect themselves from the growing health threat of wildfire smoke and what health systems can do to protect the most vulnerable. Our focus on low socioeconomic status provides unique insights into social barriers, such as legal and financial interactions with landlords. Eliciting the patients’ points of view provides insights into their social and behavioral context that are critical when planning a community-based or public health intervention.30 The 3 most relevant existing studies are summarized here:
1. Seale et al conducted 20 interviews with people with obstructive lung disease living in bushfire-prone regions of Australia to ask specifically about barriers to mask use during wildfire events. They revealed knowledge as the primary barrier, despite masks being widely used during the pandemic, and called for better communication from experts about why, how, and when to use masks during wildfire events.28 Our findings were broader and focused on other interventions besides masks.
2. Hoshiko et al from the Department of Public Health conducted a cross-sectional survey of 106 medically vulnerable people living in a rural county in California. While respondents reported taking on average 5 “actions” to reduce smoke exposure, such as wearing a mask, turning on an air cleaner, changing their daily activity, and using additional medications, approximately half (47%) reported lacking confidence in how to successfully protect their health from smoke.29 We interviewed a more geographically diverse patient population compared to Hoshiko et al but have some of the same findings.
3. Humphreys et al performed focus groups with residents and key informant interviews with local health/social service staff in Washington state. They reported the need for training health care workers to communicate effectively to the public, forming critical links between scientific/health care organizations and the public for accurate communication about health risk, and prosocial interactions among community members and organizations to prepare for and manage the aftermath of wildfire events.11 We performed individual interviews instead of focus groups, but some of the same themes emerged.
There are several notable strengths and limitations of our study. We leveraged the Kaiser Permanente integrated health network located near historically large wildfires. We recruited diverse patients, in terms of race/ethnicity and geography, as well as patients who had a vast range of experience regarding wildfire smoke exposure. The Kaiser Permanente Northern California member population is similar in demographic characteristics compared to the background population in Northern California, which speaks to the generalizability of the findings.31 However, patients who participate in the Kaiser Permanente health plan may have more trust in their health system, given that the organization typically retains 80%–90% of its members with COPD over a 5-year period. Thus, their views may differ from the general population in terms of the extent to which they wish to be contacted by their clinician or health plan. We were able to recruit participants extremely quickly (<1 month) without “cold calling” people, which is likely owed to the broad effort we made in mailing >2000 packets but could also suggest enrichment for participants who are interested or knowledgeable about the topic, such as the retired firefighter. Due to funding limitations, we could only include English speakers.32 We were not able to extract pulmonary function data to confirm airway flow limitation.
Conclusion
This study fills a critical translation gap identified by the American Thoracic Society and National Institutes of Health15,33by eliciting insights directly from high-risk patients. This study identifies several important themes that can be used to design successful interventions that will promote uptake of wildfire smoke exposure mitigation strategies. As we grapple with climate change, this information can be used by health care systems, public health entities, and clinicians to lead interventions, educational efforts, and policy reforms that improve wildfire smoke preparedness for high-risk patients. Clinicians can utilize this information and potentially address the risks of poor air quality in high-risk patients in clinic, which has not traditionally been addressed by clinicians at office visits.
Acknowledgements
Author contributions: NH, MD, and LCM conceived the idea and LCM obtained funding for the study. CML, KAD, MM, SA, AA, and LCM contributed to the design of the study. CML and KAD prepared study materials, coordinated International Review Board submission and weekly progress meetings where critical decisions were made relative to study design, and prepared the manuscript for submission. NP contributed to the production of the eligible patient dataset. JY collected and analyzed the data under guidance from LCM, with input from CML and AA. JY drafted the first version of the manuscript. All authors contributed to the interpretation of the data and the revising and approval of the manuscript.
Declaration of Interest
The authors declare that they have no competing interests.