Running Head: Impact of CTS Guidelines for SITT Use in Canada
Funding Support: This study was sponsored by AstraZeneca. AstraZeneca was involved in the review of selected literature sources for appropriateness in the context of the Canadian COPD population but had no role in the data analysis. AstraZeneca was also involved in manuscript review. Authors were involved in validating assumptions, sources, and interpreting results of the present work.
Date of Acceptance: March 2, 2026 | Published Online Date: March 30, 2026
Abbreviations: ABX=antibiotics; AECOPDs=acute exacerbations of COPD; AVOIDEx=Impact of AVOIDing EXacerbations of COPD; COPD=chronic obstructive pulmonary disease; CTS=Canadian Thoracic Society; ED=emergency department; ETHOS=Efficacy and Safety of Triple Therapy in Obstructive Lung Disease; EXACOS=Exacerbations of COPD and their OutcomeS; FEV1=forced expiratory volume in 1 second; FEV1 %pred=FEV1 percentage predicted; GOLD=Global initiative for chronic Obstructive Lung Disease; HCRU=health care research utilization; ICS=inhaled corticosteroid; IMPACT=Informing the Pathway of COPD Treatment; IP=inpatient admission; LABA=long-acting beta2-agonist; LAMA=long-acting muscarinic antagonist; MITT=multiple inhaler triple therapy; NNT=number needed to treat; OCS=oral corticosteroid; OP=outpatient visit; SITT=single-inhaler triple therapy
Citation: Bhutani M, Kaplan A, Kayaniyil S, et al. Implementation of 2023 Canadian Thoracic Society guidelines for single-inhaler triple therapy could reduce exacerbation and mortality rates in COPD: PROMETHEUS Canada. Chronic Obstr Pulm Dis. 2026; 13(3): 184-194. doi: http://doi.org/10.15326/jcopdf.2025.0687
Online Supplemental Material: Read Online Supplemental Material (255KB)
Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive and debilitating lung disease caused primarily by inhaled exposure to lung irritants, such as cigarette smoke, which accounts for 80%–90% of cases.1,2 According to the 2019 Global Burden of Disease study, COPD is the 5th ranked cause of death in Canada and the 6th ranked cause of death and disability combined.3,4 It is estimated5 that there are at least 2 million diagnosed patients with COPD in Canada with an increasing prevalence observed from 7.1% in 2000 to 9.5% in 2012. In addition to impaired respiratory function and associated mortality/morbidity, people with COPD are also more likely to develop other chronic diseases such as cardiovascular disease, anemia, metabolic diseases, osteoporosis, mental health diseases, and sleep disorders.2
The cost burden of COPD is significant; a study6 of spirometry-confirmed patients with COPD in Canada found the average annual COPD-related cost per patient was $4147. Another study evaluated the excess economic burden of COPD in British Columbia and found that having COPD led to $5196 in excess costs per person, per year over a 15-year period.7 A cost projection model conducted in Canada8 estimates that the annual societal cost of COPD will be CA$7.33 billion in 2035. Acute exacerbations of COPD (AECOPDs) are defined as a worsening or increase in respiratory symptoms that require additional treatment, and they represent a large driver for health care resource utilization.9 A study found that 37.5% of patients experiencing an exacerbation were admitted to the hospital.10 While all-cause hospitalization rates have declined in Canada, hospitalizations due to COPD increased11 by 68.8% between 2002 and 2017. Another study evaluated patients with COPD admitted to the emergency department (ED) and found that 9.5% of patients went on to develop short-term serious outcomes (defined as death, admission to a monitored unit, intubation, noninvasive ventilation, myocardial infarction, or relapse with hospital admission).12
Treatment for moderate AECOPDs typically involves treatment as an outpatient with oral corticosteroids (OCSs) and/or antibiotics. Severe AECOPDs are defined as events requiring hospitalization or ED visits. The Global initiative for chronic Obstructive Lung Disease (GOLD) report recently modified its prior ABCD classification to consolidate C and D into a new class called GOLD Group E to shift the focus to the importance of exacerbations for these patients.9 The 2025 GOLD report recommends Group E patients receive dual therapy (long-acting beta 2- agonists [LABAs]+ long-acting muscarinic antagonists [LAMAs]) initially unless eosinophil counts are higher than 300 cells per microliter, whereby triple therapy (LABA+LAMA+ inhaled corticosteroids [ICS]) can be considered. Alternatively, the 2023 Canadian Thoracic Society (CTS) COPD guidelines recommend triple therapy, and preferably single-inhaler triple therapy (SITT), as a first-line treatment for patients with impaired lung function (forced expiratory volume in 1 second [FEV1]<80%) experiencing moderate to severe symptoms, poor baseline health status, and who are at a high risk of future exacerbations.13 The CTS placed high preference on the prevention of AECOPDs and reduction of mortality independent of the eosinophil level.
While there are no pharmacologic differences between SITT and multiple-inhaler triple therapy (MITT), the majority of efficacy studies for triple therapy have been done using single- inhaler devices, thus comparable efficacy should be cautiously extrapolated to multiple-inhaler therapy options. One notable study comparing MITT and SITT in a Spanish COPD population found that those receiving SITT had a 33% reduction in mortality compared to those receiving MITT.14 Further rationale to support the use of SITT combinations include higher rates of therapy persistence, fewer inhaler handling errors, improved health status and lung function, and reduced exacerbation and mortality rates.13-16
While the 2023 CTS pharmacotherapy guidelines recommend triple therapy, and preferably SITT, more proactively in patients with moderate to severe symptom burden and high future risk of exacerbations, the long-term clinical impact of broader SITT use in Canada has not yet been studied. We aim to quantify the 10-year impact of CTS guideline-directed SITT use in the Canadian COPD population.
Methods
Model Approach
The basis of the Canadian model was developed using the PROMETHEUS study, which modeled the increased use of SITT in a U.S. COPD population.17 We developed a multi-year stochastic model that projects outcomes over a 10-year period (2025–2034) while incorporating new COPD entrants into the model yearly and allowing for multiple modeling scenarios. The model measures the outcomes on moderate and severe exacerbations and their corresponding medical costs (excluding additional SITT costs and other inhaled drug costs) and mortality. Costs were calculated using data available from the Impact of AVOIDing EXacerbations of COPD (AVOIDEx) study that categorized 2021 per-exacerbation moderate and severe costs ($460 and $11,000, respectively).18 Those costs were then adjusted each year based on Canada’s consumer price index, starting from their 2021 values and continuing throughout the 10-year duration of our model.
In our model, we simulated patients that represent the real-world Canadian COPD population and are assigned literature-derived characteristics (i.e., age, gender, incidence, changes in COPD severity, treatment, mortality, and exacerbations) accordingly. Appendix A in the online supplement outlines the characteristics applied to the COPD patient population and includes the literature-based sources used for each.
Based upon the percentage of predicted FEV1, we assigned patients to GOLD stage 1–4 classes. The progression of a patient’s COPD severity was assessed by applying a decline in FEV1, and this progression was evaluated on an annual basis.
Simulation Overview, Model Populations, and Simulation Scenarios
We based this model on the U.S. research conducted to estimate the impact of an increase in SITT utilization in the PROMETHEUS: Long-Term Exacerbation and Mortality Benefits Implementing Single-Inhaler Triple Therapy in the U.S. Population study.17 We list the specific literature sources used for baseline model patient characteristics in this model in Appendix A in the online supplement. Of note, the model is based on the Efficacy and Safety of Triple Therapy in Obstructive Lung Disease (ETHOS) study and assumptions on efficacy were made using the ETHOS, Informing the Pathway of COPD Treatment (IMPACT), and PROMETHEUS studies. We developed a multi-year stochastic microsimulation model that evaluated an increase in SITT utilization, per CTS guidelines, modeling 1000 simulations over 10 years from 2025 to 2034. After establishing the baseline population, annual adjustments to patient characteristics were made based on probability. Using literature-based assumptions (described in more detail in Appendix A in the online supplement), annual changes in patient characteristics were determined based on the probability of events such as FEV1 decline, which was modeled to represent COPD disease progression, smoking cessation rates, changes in COPD medication, moderate and severe exacerbations, and mortality. FEV1 decline and mortality were greater in patients who did not quit smoking, as well as those who had moderate or severe exacerbations. Detailed information on the yearly assumptions is described in Appendix A in the online supplement. Medication therapy was also modeled to change from baseline based on disease progression and exacerbations. Baseline medication assumptions were derived from the U.S. PROMETHEUS study in combination with AVOIDEx.17,18 Newly diagnosed (incident) patients with COPD were added each year, while some patients exited annually due to death or upon reaching 100 years of age.
We modeled 2 scenarios – “Status Quo” and “Increased SITT.”
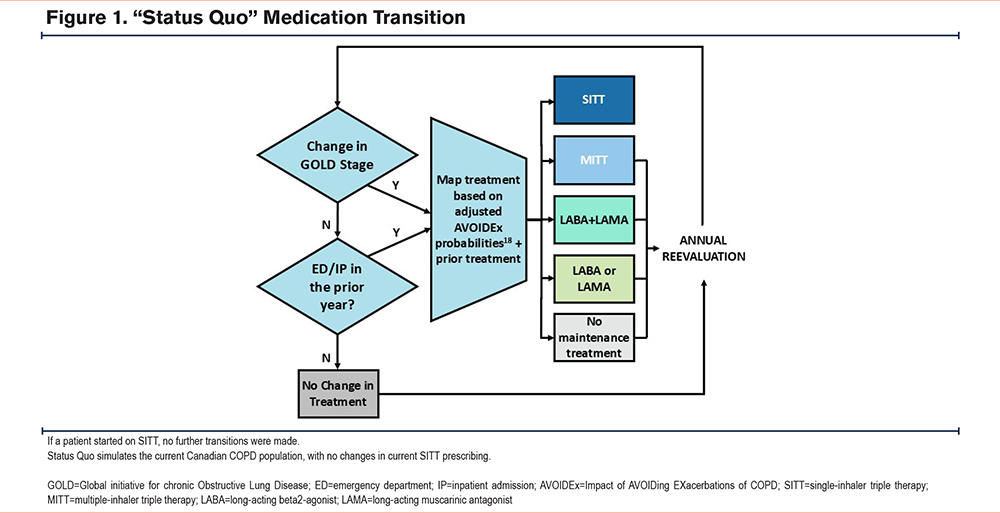
Status Quo
(Baseline): this model simulated the current Canadian COPD population, with no changes in current SITT prescribing (Figure 1).
Increased SITT
This model assumed more progressive SITT prescribing occurring over 10 years which will transition more patients to SITT according to CTS guidelines (Figure 2). Specifically, any patient with an FEV1 < 80% with either: (1) at least 1 hospitalization/ED visit, or (2) at least 2 outpatient exacerbations requiring OCSs or antibiotics would automatically initiate SITT. Additionally, any patient on MITT would transition to SITT. This model also assumes more progressive dual therapy prescribing according to CTS guidelines, transitioning patients with an FEV1< 80% who did not meet the criteria for SITT assignment to LABA+LAMA.
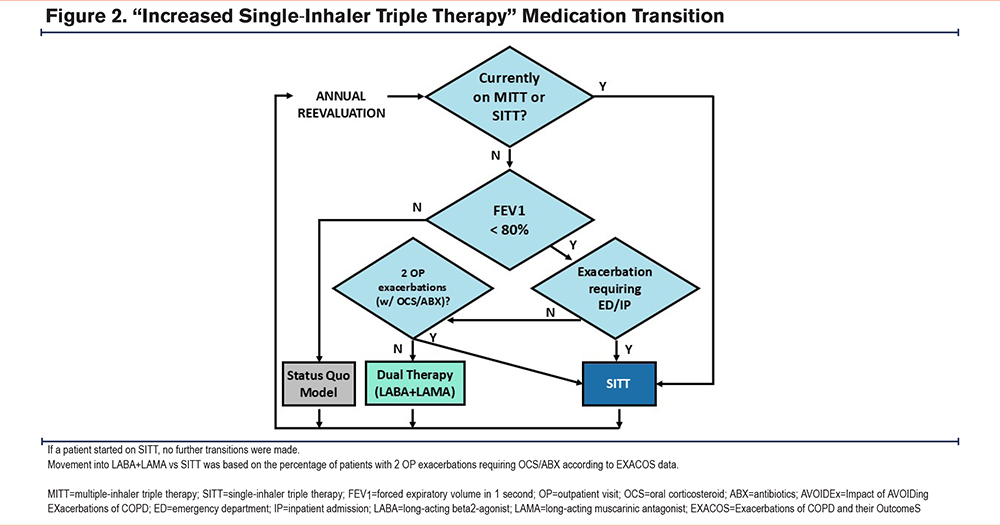
Assumptions used in the “Increased SITT” modeled population are largely the same as those used in the “Status Quo” population, with the addition of another annual medication change algorithm that transitions additional patients exclusively to SITT instead of MITT. While the CTS guidelines also recommend treatment escalation from LABA+LAMA to SITT based on persistent symptoms, this was not captured in the “Increased SITT” model due to a lack of symptom data.
We reported results for 2 populations within each scenario: total and flagged. The flagged population represents the subset of the total population that met the criteria for SITT prescribing according to CTS guidelines, independent of the actual modeled medication use for those patients. These patients represent the more severe subset within the total population. Patients with an FEV1< 80% who did not meet the criteria for SITT assignment were assigned to dual therapy (LABA+LAMA) in the “Increased SITT” model but are not included in the flagged population. This cohort influenced outcomes within the nonflagged population, contributing to differences across the total populations between the “Status Quo” and “Increased SITT” models. Additionally, since each scenario was simulated separately, the modeling approach may result in further slight variations in the outcomes for the nonflagged population.
Statistical Analyses
In the 10-year model, we projected deaths and rates (and counts) of severe and moderate exacerbations for both the total population and the flagged population under the "Status Quo" and "Increased SITT" models. Additionally, we assessed the changes in mortality, life years, and exacerbation rates and counts between the 2 models for both the total and flagged populations separately. Furthermore, we calculated the number needed to treat (NNT) in the "Increased SITT" model to extend life expectancy by one year.
Results
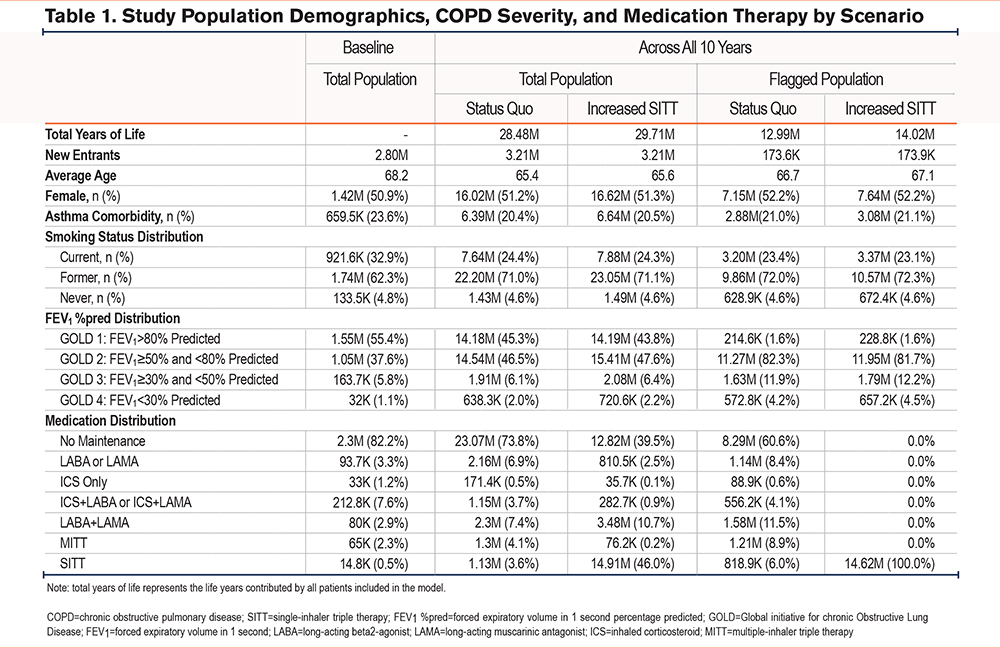
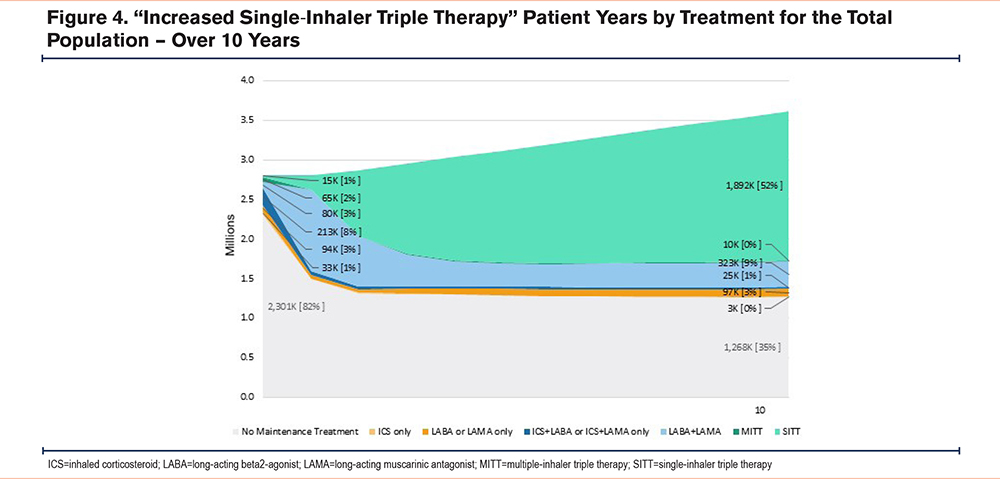
Baseline demographics are shown in Table 1, displaying an overview of the study population at year 0, prior to sampling, and across all 10 years of the study. At year 0, which represents the start of our modeling, the average age was 68.2 and 50.9% were female, representing approximately 2.80 million total years of life. Most patients were former smokers (62.3%), followed by current smokers (32.9%). Regarding the severity of the baseline population, the majority of patients, 55.4%, had an FEV1 >80% of predicted (mild COPD), followed by 37.6% with an FEV1 ≥50% and <80% of predicted, 5.8% had an FEV1 ≥30% and <50% predicted, and 1.1% had an FEV1<30% predicted (very severe COPD). In terms of the baseline medication use, the largest group of patients (82.2%) did not receive any maintenance therapy. Of the remaining patients receiving pharmacotherapy, 3.3% of patients received LABAs or LAMAs, 1.2% received ICSs only, 7.6% received either ICSs+LABAs or ICSs+LAMAs, 2.9% received LABAs+LAMAs, 2.8% of patients were on triple therapy – 2.3% on MITT and 0.5% on SITT.
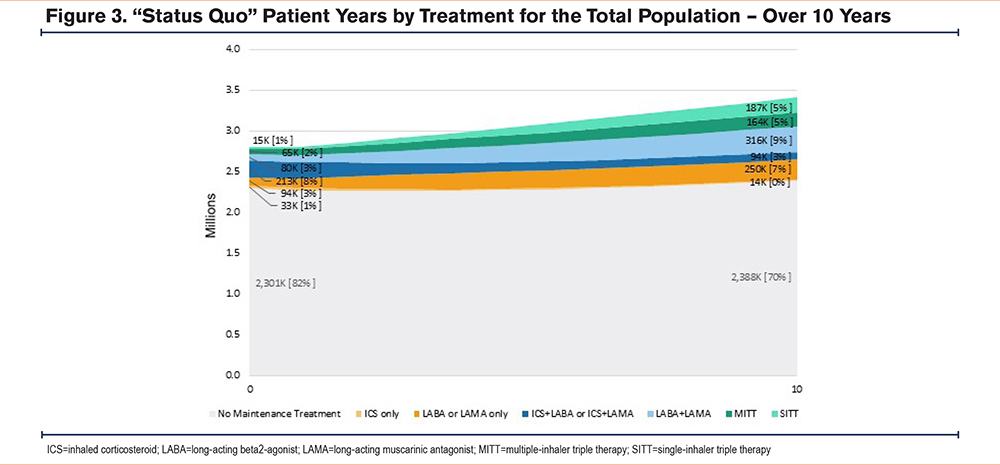
Figures 3 and 4 illustrate the changes in medication therapy used by patients over the modeled 10-year duration of the study. By the end of the study, the “Status Quo” model showed 5% of patients were on SITT, whereas the “Increased SITT” model demonstrated a significant increase, with 52% of patients using SITT. In addition, the proportion of patients receiving no maintenance treatment decreased substantially between the “Status Quo” and “Increased SITT” model. In the “Status Quo” model, 70% of patients received no maintenance therapy compared to 35% of patients in the “Increased SITT” model at the end of year 10.
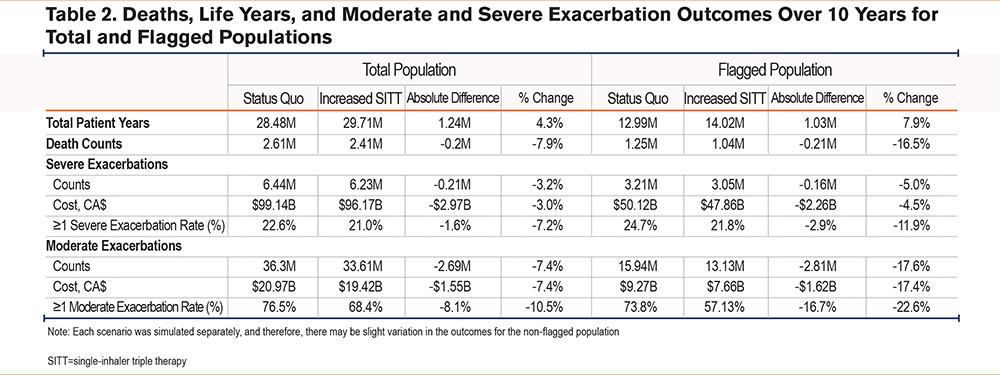
Over the 10 years modeled, the “Increased SITT” flagged population demonstrated a reduction in the severe exacerbation count of 159,000 exacerbations, equating to a savings of CA$2.3 billion as shown in Table 2. Additionally, moderate exacerbations in the “Increased SITT” flagged population were reduced by 2.81 million, which would save CA$1.6 billion. This results in total cost savings of CA$3.9 billion due to reduced exacerbations in the flagged population. Additionally, mortality decreased, with deaths reduced by 7.9% in the total population and by 16.5% in the flagged population.
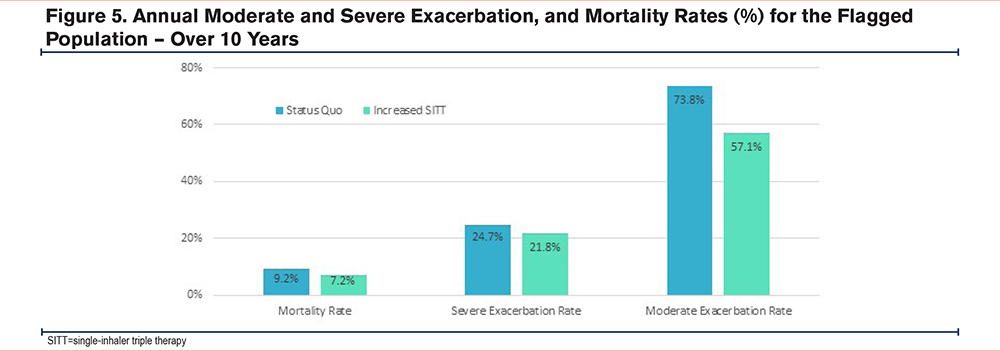
The reductions in outcomes in the total population are largely driven by reductions observed in the flagged population, with further differences attributable due to the additional LABA+LAMA assignment in the “Increased SITT” model. Because the flagged population is a subset of the total population that qualifies for progressive SITT use, it presents a more severe patient population and demonstrates greater benefits from the “Increased SITT” model. Figure 5 displays the reduction in mortality rates from 9.2% in the “Status Quo” model to 7.2% in the “Increased SITT” model, for the flagged population, indicating a 21.9% reduction. Additionally, the severe exacerbation rate decreased from 24.7% in the “Status Quo” model to 21.8% in the “Increased SITT” model, representing a 11.9% rate reduction for severe exacerbations. Furthermore, the moderate exacerbation rate for the flagged population dropped from 73.8% in the "Status Quo" model to 57.1% in the "Increased SITT" model, indicating a 22.6% reduction.
We calculated the remaining life years for patients and added life years per COPD patient, categorized by age band. Overall, the average number of life years added was higher for the flagged population under the “Increased SITT” model. All patients under 80 experienced an addition of at least 1 life year in the flagged population (Supplemental Figure 1 in the online supplement). Younger patients in the flagged population had greater increases in the number of life years added – the years of life remaining was extended 2.6 years for ages 41–50, 2.3 years for ages 51–60, 1.9 years for ages 61–70, and 1.3 years for ages 71–80, and 1 year or less for those over 80. Over the 10-year modeling period, the number of patients that needed to be treated to extend the average patient’s life by 1 year was 16 for the total population and 8 for the flagged population.
Sensitivity Testing
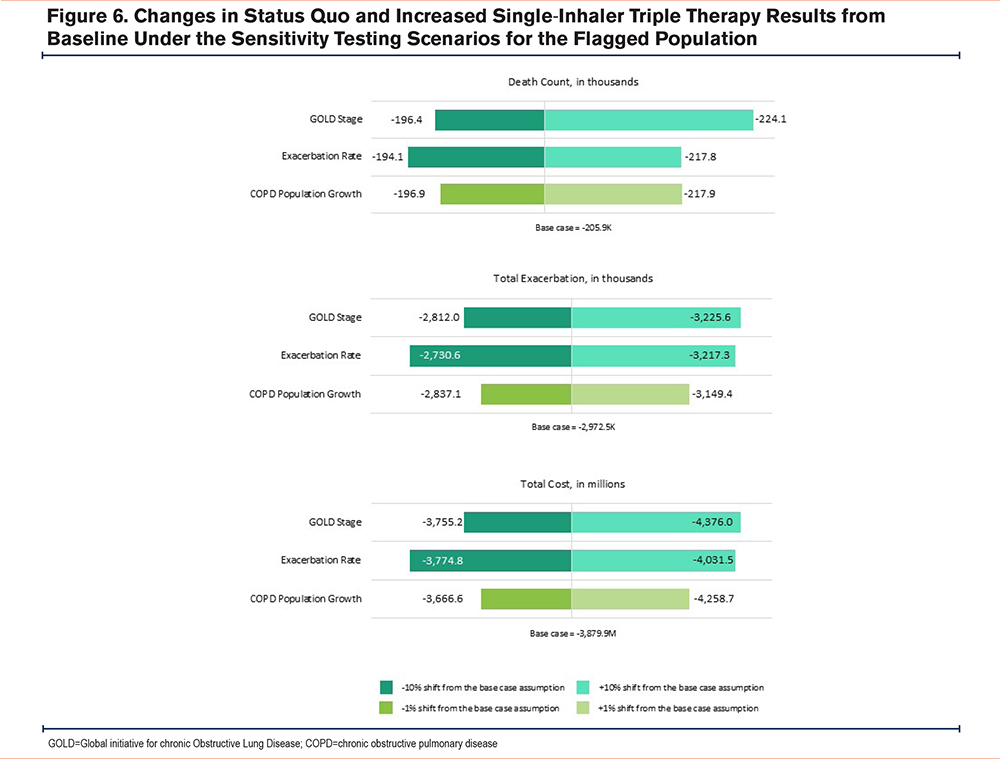
We conducted sensitivity testing to understand the impact of variations in our assumptions on our “Increased SITT” death and exacerbation count, and exacerbation cost outcomes. We tested 3 variables: (1) the baseline GOLD stage distribution, (2) the exacerbation rates, and (3) the incidence rate/population growth.
For the GOLD distribution, we assumed that the COPD population was more or less severe than the baseline population by changing the distribution of the baseline GOLD distribution for stages 1 through 4 by 10% overall. For the more severe scenario, we reduced the proportion of patients with COPD in GOLD stage 1 and increased the proportion of patients with COPD in GOLD stages 2 through 4. On the other hand, the less severe scenario reflected more GOLD stage 1 patients and fewer GOLD stage 2 through 4 patients. For the exacerbation rate sensitivity testing, we took the baseline exacerbation rates and increased or decreased them by 10%. We applied this factor separately to the 1 and 2+ moderate and 1+ severe exacerbation baseline rates. For the incidence rate/population growth scenario, we adjusted the baseline rate of 2% by increasing it by 1% (to 3%) and decreasing it by 1% (to 1%).
Figure 6 displays the change in “Status Quo” and “Increased SITT” results in the flagged population under the sensitivity analysis for the 3 varying assumptions described above. We found that making the COPD population more severe by assuming more patients in higher GOLD stages had the most significant impact on the results. This effect was observed across both the total and flagged populations, as well as in both modeled scenarios, “Status Quo” and “Increased SITT.” In the flagged population, assuming a more severe COPD population by changing the GOLD stage distribution overall by 10% leads to more patient life years being incorporated into our model. This change results in higher reduction in death counts and severe and moderate exacerbations due to increased SITT compared to status quo. In addition, a 10% increase in the base case exacerbation rate had a significant impact on the reduction in death counts, moderate exacerbations, and costs due to increased SITT compared to status quo. Altering the assumptions for COPD incidence rates (or population growth) had the smallest impact on the results across all populations and modeled scenarios. Further details on the impacts of assumption changes are also provided in Supplemental Table 1 in the online supplement.
Limitations
Information on clinical markers, including blood eosinophil count and symptom severity (such as COPD Assessment Test and modified Medical Research Council scores), was not available and thus, was not incorporated into this model. Instead, we used the percentage of predicted FEV1 to determine COPD severity. An annual decline in FEV1 was used as a proxy for progression of severity over time. Additional FEV1 decline was applied to patients with concomitant asthma and for active smoking status. Additionally, the costs related to outpatient therapies (such as maintenance medications, oral antibiotics, or oral corticosteroids prescribed to outpatients) were not included in the overall costs. Due to availability of generic maintenance therapies, we did not model costs associated with those therapies specifically. We note that increased use of more expensive therapies, such as SITT, would overestimate the cost savings noted in this study as they are not included in our cost projections.
This study relied on several sources of literature to determine baseline characteristics and transitions over time; use of other sources could result in different results. Notably, the baseline medication distributions in this model were derived from the U.S.-based PROMETHEUS study as well as AVOIDEx, which is a Spanish study. Wherever possible, the preference was to utilize recent Canadian references in our assumptions. In cases where Canadian data was unavailable, we carefully reviewed and utilized alternate sources to ensure appropriateness in the Canadian COPD population. Sources were compared to the Canadian population and were vetted by several authors who are subject matter experts and practice in Canada to ensure external applicability of the data. Use of Canadian claims data, while ideal, was not available for this model and would be expected to produce differing results to those presented here.
While the ETHOS study was used in this work, we note that the 1-year study is being extrapolated to a 10-year model, which may overstate potential SITT benefits as real-world patients may be less adherent over a longer time frame. Additionally, the ETHOS patient population represents patients with a prior history of exacerbations and treatment, and patients naive to treatment may behave or respond differently. Real-world adherence may also be different than noted in the trial population. Different formulations of inhaled therapies may also impact outcomes (such as use of spacers, dry-powder inhalers, etc.).
This model assumes ideal adoption of the CTS guidelines; real-world adoption may be less than ideal and may result in differing outcomes. Additionally, while the CTS guidelines recommend SITT for patients with low exacerbation risk and persistent symptoms despite adequate treatment with LABA/LAMA dual therapy, the potential benefits in this patient population are not well studied or well quantified in the current body of literature. Accordingly, our model may overestimate potential benefits to this patient population but assuming a similar benefit to patients with a higher exacerbation risk. This model assumes future benefits based on historical data and does not account for other interventions or new literature that may emerge in the future that can lower the exacerbation risk of the Canadian COPD population. Risks and adverse events related to therapy with SITT (including pneumonia) are not modeled within this study. Any alteration in the assumptions used to build the base assumptions of the model will lead to varying of the results.
Discussion
Triple therapy with SITT has been demonstrated as beneficial for patients that are considered to be high risk. While the GOLD guidelines have historically reserved triple therapies for patients who are more severe, the CTS guidelines present a more progressive approach to SITT utilization than the GOLD recommendations. The PROMETHEUS study, which this work was based on, evaluated the impact of increased SITT utilization on a U.S. population. However, the clinical impact of broader SITT use for patients with COPD in Canada has not yet been studied.
This model utilizes a patient population that was based on Canadian demographics obtained from the Canadian Chronic Disease Surveillance System, and baseline GOLD stage distribution was modeled on data from the Canadian Cohort Obstructive Lung Disease study, which is a national, longitudinal cohort study. Additional assumptions were based on data from several landmark clinical studies including AVOIDEx, Novel Observational Longitudinal Study, and PROMETHEUS (as described in the online supplement). The modeled status quo population had a low rate of maintenance treatment with treated patients representing only 26% of total patient years across the 10-year model. This rate of undertreatment is higher (at 74%) than we observed in similar work that is underway in several other countries (including France where the no-maintenance therapy rate was 25%, Italy where it was 6%, and Spain where it was 2%). The high rate of undertreatment observed could be a factor of slow guideline recommendation uptake. On a national level, there are several barriers to guideline implementation including but not limited to a large number of undiagnosed patients, the cross country lack of primary care providers, the lack of consultants and specialists in parts of Canada, the need for patient monitoring with therapeutic escalation as needed, lung function tests being done at a lower rate than desired due to resource limitations, lack of medication coverage, and a general inertia to change.19
Over our modeled 10 years, we estimate that an increase in guideline-based SITT utilization rates would decrease severe exacerbations by 5.0% or 159,000 exacerbations and would decrease moderate exacerbations by 17.6% or 2.81 million exacerbations in the flagged population. As exacerbations are associated with a significant health care resource burden, hospitalizations, and high costs, this reduction would lead to a cost savings of CA$3.9 billion. Additionally, deaths would decrease by 16.5% in the flagged population for a reduction of 206,000 deaths overall. The additional differences observed in the total population, beyond those attributable to the flagged population, can be explained by the assignment of LABAs+LAMAs according to CTS guidelines in the “Increased SITT” model. This approach results in 124,000 more moderate exacerbations, 48,000 fewer severe exacerbations, 1000 additional deaths prevented, and approximately CA$600 million in further cost savings, for a total of CA$4.5 billion across the total population. This translates to a NNT to extend a COPD patient’s life by one year of 16 for the total population and 8 for the flagged population. As described in our sensitivity analysis, we varied the assumptions to ensure that the overall direction of the results would not change if we had used alternate assumptions in this model.
The results presented here reinforce the benefits of SITT therapy on exacerbation reductions and mortality observed in the ETHOS and IMPACT trials. The implementation of guidelines that encourage earlier transition to SITT, such as the CTS guideline, will reduce the burden of exacerbations, which reduces mortality as well as health care resource utilization (HCRU) and cost. We note that our model and subsequent results do not factor clinical symptomatology into therapy transitions as this data was unavailable to be modeled on a population basis. Due to this limitation, the increased SITT use observed in the “Increased SITT” model is likely a conservative estimate.
While optimization of inhaled therapy can have a significant impact on patient outcomes, particularly in those patients with a higher COPD severity, this study highlights the importance of early patient diagnosis and treatment, as this data shows treatment of younger patients results in greater increases in number of life years added. Moreover, while these results only focus on the benefit of early treatment with SITT therapy, the addition of nonpharmacologic treatments early in a patient’s disease course (such as appropriate vaccinations, smoking cessation, and pulmonary rehabilitation) would serve to improve the results we present here. Implementation of these non-pharmacologic strategies that are recommended by the CTS guidelines will also serve to reduce the HCRU burden of COPD in Canada. Additionally, while this model focuses on the impact of inhaled treatments on COPD exacerbations and all-cause mortality, there is increasing recognition of the relationship between COPD, cardiovascular disease, and osteoporosis. As these benefits were also not factored into our modeling, this represents another potential underestimation of potential SITT benefits.
Conclusions
The CTS 2023 COPD guidelines simplified its treatment algorithm and shortened the path to SITT, increasing the potential utilization of that treatment option versus the previous recommendation. Our modeling suggests implementation of the CTS 2023 COPD guideline recommendation for SITT could reduce exacerbations and their corresponding heath system medical costs and extend COPD patient life.
Acknowledgements
Author contributions: MB, AK, SK, KJ, RO, JB, JC, PB, and BP, were all involved in the review of assumptions, the review of modeling results, and manuscript drafting or review.
Other acknowledgments: We thank Steven Wright for his work in building the stochastic model.
Statement of Ethics: Study approval was not required as this was a modeling study based on published literature. No human participants were involved in this work and no informed consent was required.
Data availability: Published literature was utilized for this modeling study. Details on the sources utilized for each assumption are described in the supplementary materials.
Declaration of Interest
MB is on the speakers’ bureau and is an advisor for AstraZeneca, GSK, Sanofi, Takeda, and Pfizer, and also receives research grants from CIHR, Alberta Lung, AstraZeneca, GSK, and Sanofi. AK is a member of the advisory board or speakers’ bureau for ALK, AstraZeneca, Boehringer Ingelheim, GSK, Idorsia, Merck Frosst, Pfizer, Sanofi, Trudel, and Valeo.
SK, KJ, RO, and JB are employees of AstraZeneca and may hold stock and/or stock options in the company. JC, PB and BP are employees of Milliman, which was contracted by AstraZeneca to conduct this study.
The American Academy of Actuaries requires its members to identify their credentials in their work product. BP and JC are members of the American Academy of Actuaries and meet its relevant qualification requirements.