Running Head: AATD Testing in a Large Health System
Funding Support: None
Date of Acceptance: March 15, 2026 | Published Online Date: March 30, 2026
Abbreviations: AAT=alpha-1 antitrypsin; AATD=alpha-1 antitrypsin deficiency; BMI=body mass index; CI=confidence interval; COPD=chronic obstructive pulmonary disease; EHR=electronic health record; FEV1=forced expiratory volume in 1 second; FEV1 %pred=FEV1 percentage predicted; FVC=forced vital capacity; HET=heterozygotes; ICU=intensive care unit; IEF=isoelectrofocusing; NLR=neutrophil lymphocyte ratio; OR=odds ratio; PCR=polymerase chain reaction; WBC=white blood cell
Citation: Robinson DD, Chiu CY, Hampton JI, Solomon GM, Wells JM. Clinical characteristics and health care resource utilization among individuals undergoing alpha-1 antitrypsin testing in a quaternary health system. Chronic Obstr Pulm Dis. 2026; 13(3): 227-236. doi: http://doi.org/10.15326/jcopdf.2025.0723
Introduction
Alpha-1 antitrypsin deficiency (AATD) is a genetically inherited condition that is the result of a mutation in the SERPIN1A gene, located on the long arm of chromosome 14 at 14q32.1, which leads to misfolding or absence of the antiprotease alpha-1-antitrypsin (AAT) protein.1-3 Accumulation of misfolded protein leads to liver degradation and insufficient degradation of proteases causing loss of function lung disease, leading to cirrhosis and emphysema, respectively.1,2 The clinical consequences of ZZ, SZ, and MZ phenotypes are well described.1,2 Many other variant alleles exist, but literature is scarce on the clinical significance of these mutations.1,4 Despite clear recommendations for screening, AATD remains overwhelmingly underdiagnosed with it being diagnosed in <10% of those expected based on screening studies.1,3-8 Delays in diagnosis are also common, taking up to 8.8 years from the time of symptom onset to AATD diagnosis.8 Clinical pathways and processes for AATD testing have been proposed as a means to improve screening for AATD. It is unclear how order sets to test for AATD in clinical practice will influence AATD screening and if testing for variants other than M, S, and Z provides additional utility in identifying clinically significant disease.3,6
Methods
We conducted a retrospective review on all adult patients who had AAT Pi-typing using isoelectrofocusing (IEF) (Quest Diagnostics; Secaucus, New Jersey), performed from January 2016 through December 2021 in the University of Alabama at Birmingham Health System. This test was used for several reasons, including its availability to clinical providers and ease of incorporation into order sets in the health system (e.g., hepatology clinic order set, chronic obstructive pulmonary disease [COPD] exacerbation order set). We recorded ordering location (pulmonary, hepatology, other), AAT Pi*type results, AAT levels, age, sex, race, body mass index (BMI), smoking status, comorbidities (including COPD, asthma, bronchiectasis, cirrhosis), therapies including supplemental oxygen use and augmentation therapy use, spirometry values (including forced expiratory volume in 1-second [FEV1], forced vital capacity [FVC], and FEV1 to FVC), and laboratory data (liver function tests, complete blood count, immunoglobulins). Health care utilization events of interest included outpatient visits for acute respiratory exacerbations, hospitalization for respiratory exacerbations, intensive care unit (ICU) utilization; vital status was recorded for death from any cause after a Pi*type was ordered. We then divided the cohort into the following groups based on the results of AAT testing: normal (Pi*MM, Pi*M1M2, Pi*MZ Pratt), Pi*Z-Heterozygotes (Het) (Pi*MZ, Pi*SZ, Pi*IZ, Pi*FZ), Pi*ZZ, Pi*S-Het (Pi*S?,Pi*SS, Pi*MS, Pi*CS), and defined a Pi*Non-S/Non-Z group that included other identified Pi*types (Pi*BM, Pi*CM, Pi*DM, Pi*EM, Pi*FM, Pi*GM, Pi*LM, Pi*M1N, Pi*MT). Chi-square and Kruskal-Wallis tests were used for analyses in SAS 9.4. We used generalized linear models for modeling FEV1 percentage predicted (FEV1 %pred) with Pi*type by smoking status. Logistic regression was utilized to measure associations between Pi*type and outcomes of hospitalization, ICU admission, and death with race, age, and sex. This study was approved by the institutional review board at the University of Alabama at Birmingham (UAB IRB-300006077).
Results
A total of 1777 tests were ordered from January 2016 through December 2021 in the University of Alabama at Birmingham Health Care System. AAT Pi*type testing increased each year from 129 tests in 2018 to 613 in 2021. Most tests were ordered by hepatology and pulmonary services (Figure 1). A total of 530 tests (29.96%) were ordered by pulmonary and 1068 tests (60.4%) were ordered by hepatology. Of the 1777 tests ordered, 1772 had phenotype/Pi*type results (99.7%) and 1135 (63.9%) had AAT levels ordered.
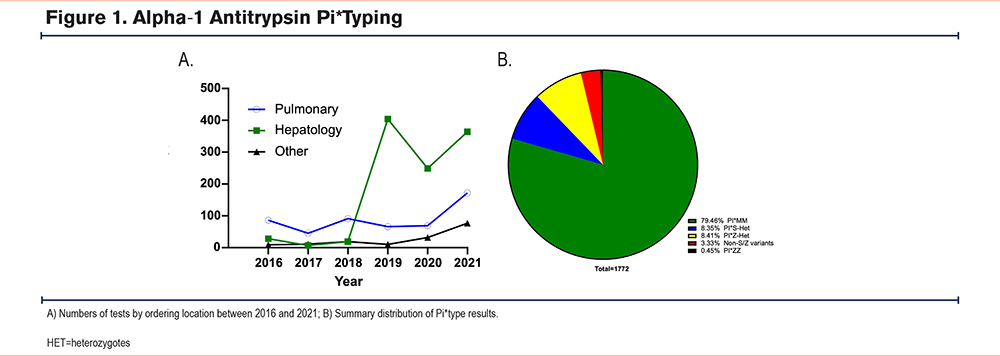
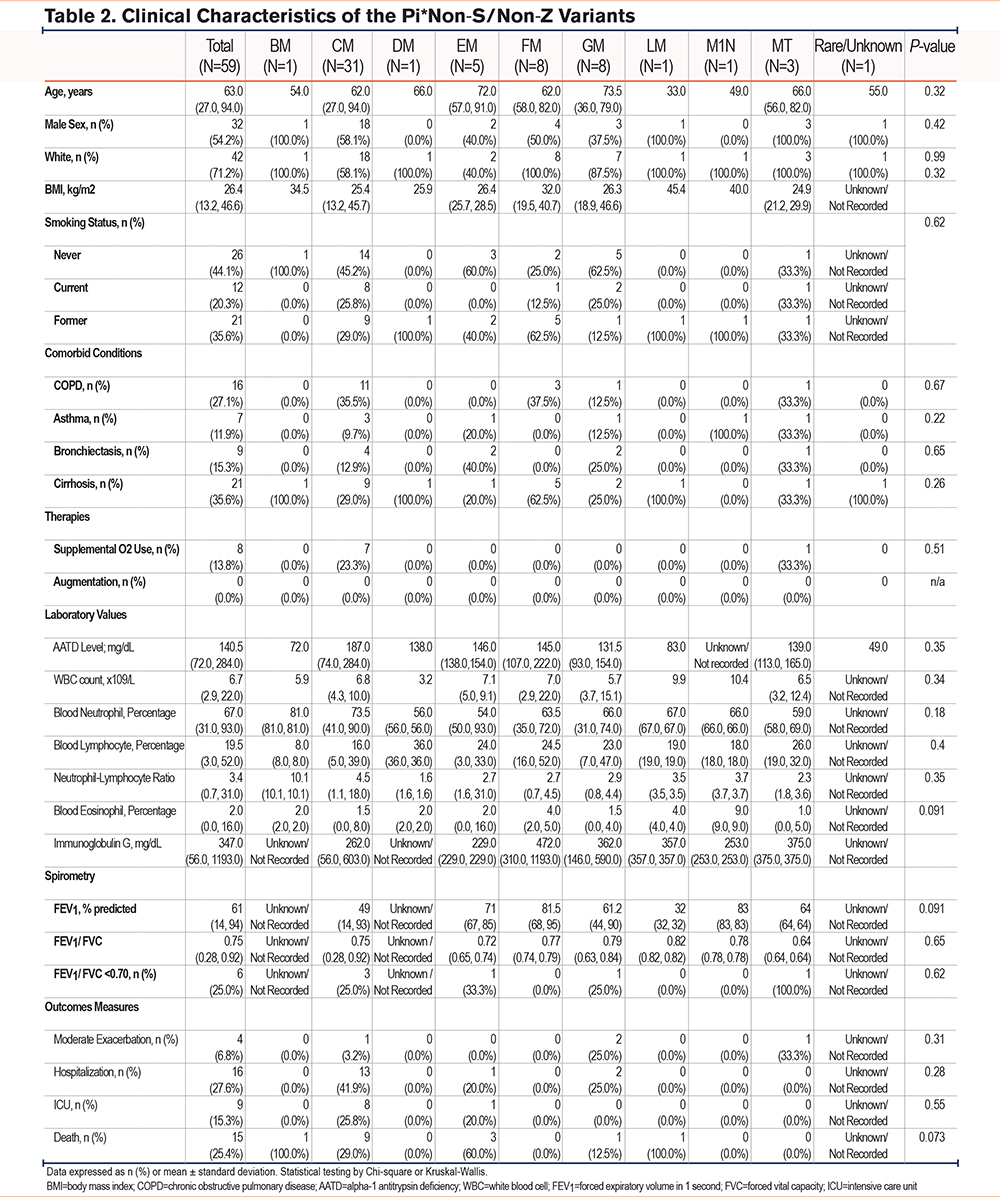
The cohort was grouped by Pi*type as follows: 79.5% normal, 8.4% Pi*Z-Het, 8.4% Pi*S-Het, 3.3% Pi*Non-S/Non-Z, and 0.5% Pi*ZZ (Figure 1, Table 1). Our Pi*Non-S/Non-Z cohort was composed of Pi*BM (1/59 [1.7%]), Pi*CM (31/59 [52.5%]), Pi*DM (1/59 [1.7%]), Pi*EM (5/59 [8.5%)]), Pi*FM (8/59 [13.6%]), Pi*GM (8/59 [13.6%]), Pi*LM (1/59[1.7%]), Pi*M1N (1/59 [1.7%]), and Pi*MT (3/59 [5.1%]) (Table 2). We then characterized the individuals with any abnormal Pi*type (n=364) identified by testing. As detailed in Table 1, individuals with any abnormal Pi*type included in the cohort were 61±15 years old, 47.5% male, 89.3% White, 6.3% Black, and 4.4% other race (Asian [0.8%], Hispanic [0.8%], other/unknown/refuse to answer/missing [2.8%]). More than half (55.3%) of the cohort were never smokers, 30.4% were former smokers, and 14.2% were current smokers. Liver disease was present in 69.5%, and COPD was present in 21.6%. Age, sex, BMI, smoking status, and asthma diagnosis were similar across groups. We observed a higher proportion of Black patients in the Pi*Non-S/Non-Z cohort (n=11, 18.6%) compared to other groups (Pi*Z-Het [n=3, 2.0%]; Pi*S-Het [n=9, 6.1%]; Pi*ZZ [n=0, 0%]; p<0.0001). In our Non-S/Non-Z cohort, 8 out of 11 of those identifying as Black were Pi*CM phenotype, 2 out of 11 were Pi*EM, and 1 out of 11 were Pi*GM (Table 2). As detailed in Table 1, we observed differences in COPD prevalence by Pi*type (P=0.03), but did not observe between-group differences in other key comorbid conditions including bronchiectasis (P=0.54), abnormal liver function tests (P=0.35), and cirrhosis (P=0.96).
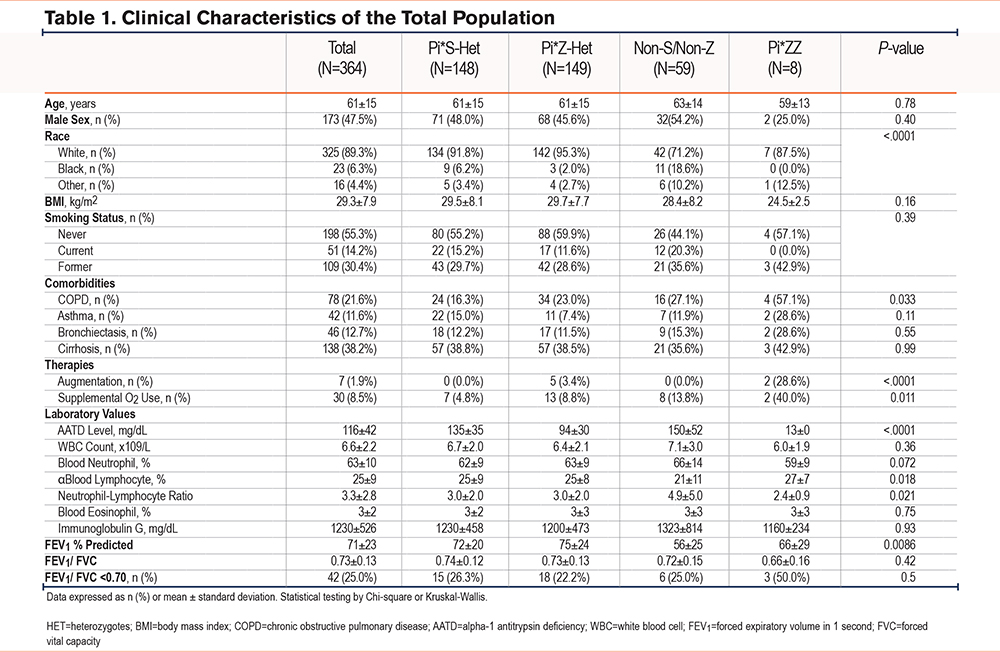
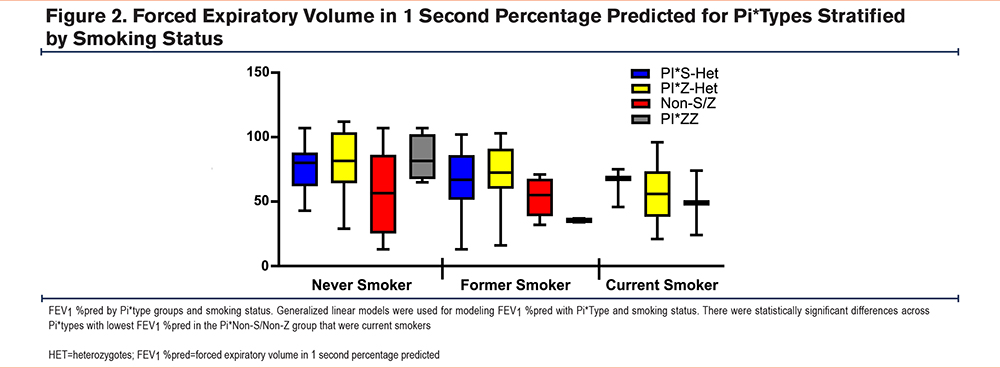
Next, we evaluated laboratory and physiological measures in the various Pi*types. The mean FEV1 %pred is statistically different among Pi*types with the lowest in the Pi*Non-S/Non-Z group (55.824.5%) followed by Pi*ZZ (65.829.3%), Pi*S-Het (72.119.7), and Pi*Z-Het (75.323.5%), P=0.0086. We then stratified lung function by smoking status. Not unexpectedly, FEV1 %pred was lowest among current smokers and highest in never smokers in the full cohort (p=0.0002). Of note, there were no active smokers in the Pi*ZZ phenotype. As shown in Figure 2, we found that FEV1 was lowest in Pi*Non-S/Non-Z in current smokers (P=0.0001), but FEV1to FVC values were similar across Pi*type groups in current or former smokers.
Mean AAT levels were lowest in the Pi*ZZ group (13.0mg/dl; n=1/8) and the Pi*Z-Het group (93.729.9mg/dl; n=111/149) but were otherwise similar across the other groups: the Pi*Non-S/Non-Z group (149.652.4mg/dl; n=28/59), the Pi*S-Het group (134.535.0mg/dl; n=92/148), and the normal group (159.039.1mg/dl; n=903/1408). We compared values of routinely measured inflammatory markers by Pi*type. While there was no significant difference in white blood cell values (Pi*Non-S/Non-Z group [7.13.0], Pi*Z-het [6.42.1], Pi*S-het [6.72.0], and Pi*ZZ groups [6.01.94] [p=0.3578]), mean neutrophil lymphocyte ratio (NLR) was highest in the Pi*Non-S/Non-Z group (4.95.0) compared to the Pi*Z-Het (3.02.0), Pi*S-Het (3.02.0), and Pi*ZZ groups (2.40.9) (p=0.021). There were no significant differences in immunoglobulin levels across subgroups.
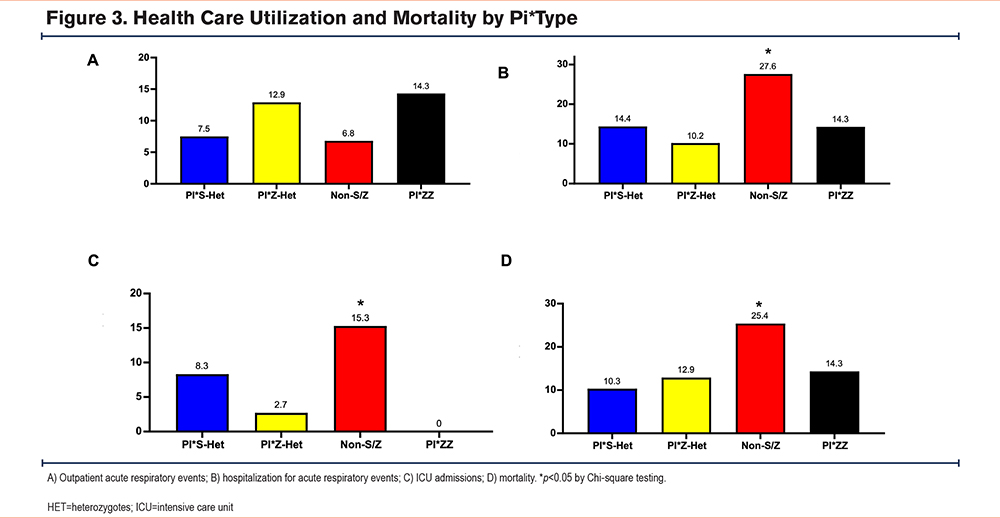
We then measured health care utilization and outcomes across abnormal Pi*types. Patients in the Pi*Non-S/Non-Z group had higher incidence of hospitalization for acute respiratory events (27.6%) compared to Pi*Z-Het (10.2%), Pi*S-Het (14.4%), and Pi*ZZ (14.3%) (p=0.018) as well as higher ICU utilization (p=0.011) and death (p=0.041) compared to the other groups (Figure 3). In order to control for confounders, we next used logistic regression analysis on the outcomes of ICU utilization, hospitalization, and mortality adjusted for age, race, sex, smoking status, and cirrhosis diagnosis. We observed an increase in odds of hospitalization (odds ratio [OR] 1.88, 95% confidence interval [CI] 0.85–4.18) as well as ICU utilization (OR 1.53, 95% CI 0.56–4.16) in the Non-S/Non-Z group compared to the Pi*S-Het group although the associations do not reach a statistical significance. Mortality was elevated in the Non-S/Non-Z group compared to Pi*S-Het (OR 3.31, 95% CI 1.41–7.76). There were similar relationships when comparing between group differences between Black or non-Black populations when adjusted for age, race, sex, smoking status, and cirrhosis diagnosis on the outcomes of hospitalization (OR 1.95, 95% CI 0.89–4.27), ICU admission (OR 1.53, 95% CI 0.57–4.10), or mortality (OR 3.06, 95% CI 1.32–7.11).
Discussion
We observed that rates of testing for AATD using Pi*typing increased substantially over time within a quaternary health care system, and uncommon mutations were associated with clinically relevant outcomes. Our findings emphasize the importance of testing for AATD and that detection of clinically significant AATD disease phenotypes are under-recognized. The increase in testing over time in our health system was largely due to implementation of AAT screening into commonly used electronic health record (EHR) order sets developed as part of process improvements for new patients being evaluated by the hepatology clinic and in the COPD exacerbations order set starting in 2019. Multiple prior attempts to increase AATD testing have been proposed by others in the past with varying results, but our findings suggest there is work still to be done.9-12 In 2020, there was a decrease in the number of orders, likely related to the COVID-19 pandemic, as the amount of testing increased again in 2021.
In parallel with the increase in tests performed, we observed an increased number of abnormal alleles and were able to identify a group of non-S, non-Z individuals we designated as a Pi*Non-S/Non-Z group. The low number of observations of the non-S, non-Z Pi*types are not surprising and are consistent with previously reported rates.13 This Pi*Non-S/Non-Z group, despite being composed of heterogeneous Pi*types, had clinically meaningful markers of disease severity including lower FEV1, higher rates of hospitalization for respiratory events, higher ICU utilization, and death during the time period of our study compared to other Pi*type groups, signifying a potential clinical association more substantial than what has been previously recognized.13 This Pi*Non-S/Non-Z group also had a higher NLR, suggesting a potential heightened inflammatory state in this group.14 A higher NLR is associated with indices of COPD disease severity and is predictive for COPD exacerbations.15 Higher NLR in the Pi*Non-S/Non-Z cohort may explain the higher rates of respiratory event hospitalization and ICU admission, though these results need to be confirmed.
Although modeling has not identified associations between these Non-S/Non-Z Pi-types and either antineutrophil elastase activity or misfolding, these data suggest the possibility that rare AAT mutations could influence disease risks through other mechanisms.13,16-20 One consideration could be altered regulation of inflammation, supported by the higher NLR in this cohort.14 Another consideration for the observed differences in clinical outcomes by race and Pi*type suggest that social determinants of health may also play a role. The fact that nearly 20% of the Pi*Non-S/Non-Z group were Black is an important observation. The most common Non-S/Non-Z variant was Pi*CM (52%), and this variant had a higher proportion of Black participants (72% of Black patients with the Non-S/Non-Z phenotype had the Pi*CM variant). Given the higher proportion of Black patients with Pi*CM variant, future studies should explore these associations in a prospective manner. The exact implications for this finding are unclear, but it reinforces the need to test all individuals at risk for AATD, regardless of race. Many patients would not have been diagnosed if not for IEF testing. Therefore, performing phenotyping rather than simple genetic screening and obtaining levels may be important for those populations known to have lower AATD prevalence, particularly in those without risk factors such as cirrhosis or COPD. Black individuals are a population known to have proportionally lower AATD testing compared to other genetic ancestry groups.21 Recently, Riley et al demonstrated that White race is a factor favoring increased AAT testing, and non-White race as having lower odds of AAT testing.22 By predominantly testing individuals with European ancestry, the medical community may be missing other populations at risk for adverse health outcomes.
Our observed testing practices prior to 2019 reflect previously reported findings, with pulmonologists ordering the most tests, followed by hepatologists, and then other specialties (primary care, surgery, etc.). For example, in the National Detection Program for AATD, more than 580,000 individuals were assessed for AATD from 2003-2017, and pulmonologists were more likely than primary care providers to test for AATD.23 However, with inclusion of AAT Pi*typing as part of a new patient order set for the chronic liver disease clinic, hepatology surpassed pulmonology as the service line that ordered the most AAT phenotype tests.
Over the 6-year timeframe of our trial, we identified 8 of 364 (2.2%) Pi*ZZ individuals, which is similar to previously reported rates.9,24 Several strategies have been proposed to improve testing for AATD, all with varying levels of success. Schumacher et al used a web-based education module to improve awareness of AATD screening with a nearly doubled rate of high-risk screening, including more than one fourth of those tested identified as having AATD.17 EHR systems have been used in the past, with Choudry et al using the EHR database at 2 clinics to identify patients diagnosed with COPD and arrange AAT testing, with 109 patients coming for testing out of a total of 1247 COPD patients identified.12 Another study by Jain et al used their EHR to alert physicians to order AAT testing of patients with obstruction on pulmonary function testing, with testing completed on 209 patients out of a total of 12,369 identified as eligible for testing.10 Using their EHR systems, these 2 studies were able to identify 1 out of 109 (0.9%) and 1 out of 46 (2.17%) patients with Pi*ZZ homozygote, respectively.10,12 While using EHR systems and use of order sets are clearly helpful to increase testing, it is unknown if using EHR order sets will consistently identify phenotypes that will manifest clinically relevant disease.
There are many methods available for testing for AATD, including immunoassays (radial immunodiffusion, rocket immunoelectrophoresis, and nephelometry), phenotyping using thin-layer isoelectricfocusing, and genotyping using either polymerase chain reaction (PCR) or sequencing of exonic DNA.25 While immunoassays are relatively cheap, they do not reliably detect heterozygotes.25 Our population was identified using IEF, but null variants cannot be detected using this method, which is a limitation of the IEF approach. Pi*typing using IEF is advantageous for health care systems as it can detect an AAT allele without knowing the AAT level, but it is a manual technique which requires skills and appropriate standards for testing.25 Genotype testing has the advantage of being relatively inexpensive and definitive if using an available primer, but may miss rare variants unless using sequencing, which is expensive.25 Genotype testing is recommended as a first line testing method due to its ability to provide accurate and early identification of the traditional disease-causing alleles (S or Z) followed by confirmatory AAT level testing and consideration of alternate testing (i.e., IEF) when there is a discordance between the level and genotype.26 Although genotype testing is recommended as first-line screening, our findings suggest that phenotyping should not be limited to having a discordance between the level and the genotype because almost all Non-S/Non-Z phenotypes will have normal levels. If IEF testing were done for discordance between levels and genotype testing, only 2–3 patients would have been identified out of the 59 patients in this study and, therefore, an important group of patients would have gone unrecognized. One potential solution based on these findings would be to include the Pi*CM variant in genetic PCR testing because the majority of Pi*Non-S/Non-Z patients were the Pi*CM variant in our study. Health systems should be cognizant of these differences when selecting the appropriate test for their use case.
Our study is not without limitations. Most importantly is the single-center design and lack of a validation cohort. Additionally, given that the majority of testing for AATD was done in the hepatology clinic as part of diagnostic evaluation for liver disease, cirrhosis and abnormal liver function testing were likely overrepresented and, therefore, the results of our cohort may not be as applicable to the general AATD population. In fact, cirrhosis was more common (38.2%) in our cohort, compared to reported prevalence27 of cirrhosis in Pi*ZZ AATD, which is typically just over 10%. Regardless of the high prevalence of concomitant liver disease in our cohort, cirrhosis was not significantly higher in the Pi*Non-S/Non-Z group compared to the other groups, so a finding of end-stage liver disease alone would not explain higher observed rates and numbers of hospitalization, ICU utilization, or death observed in the Pi*Non-S/Non-Z group. Our data is limited by the retrospective nature of the study and small numbers of Pi*ZZ genotypes. The small sample size and heterogeneous nature of the Non-S/Non-Z grouping schema limit investigations into associations between individual rare allelic combinations and clinically relevant disease in this cohort. However, these findings present an opportunity for groups of clinicians and researchers in the alpha-1 community to collaborate to create research registries – like those that are done within the Alpha-1 Foundation28 or through the European Alpha-1 Research Collaboration.29
In summary, our experience of screening for AATD using Pi*phenotyping as part of an EHR-based order set increases the number of tests. This strategy not only identified individuals with severe AATD, but also recognized a heterogeneous group of non-S, non-Z individuals who are linked with relevant clinical outcomes. While these findings need to be replicated in future studies, our results underpin the need to explore relationships between rare allelic combinations and clinical outcomes.
Acknowledgements
Author contributions: Conceptualization of the study was provided by DDR and JMW. DDR, C-YC, GMS, and JMW provided study methodology. Data collection was completed by DDR and JIH. DDR and JMW wrote the original draft of the manuscript with all authors editing, reviewing, and approving the final version submitted for publication.
Declaration of Interest
DDR, CYC, and JIH have no conflicts to declare.
GMS reports receiving grants from the Cystic Fibrosis Foundation, the National Institutes of Health, the COPD Foundation, the PCD Foundation, Vertex, Electromed, Boeringer-Ingelheim, 4DMT, BIOMX, Astra-Zeneca, and Sanofi for work unrelated to the current manuscript. GMS has received honoraria for consulting work from Insmed, Electromed, and Vertex for unrelated projects.
JMW reports grants and contracts to his institution from the National Institutes of Health, Veterans Affairs, Medscape, Verona Pharma, and Sanofi. JMW has served as a consultant for AstraZeneca, Takeda, Bavarian Nordic, Krystal Biotech, Sanofi, and Verona Pharma for content outside the submitted work.