Running Head: Association Between Symptom Changes and COPD CARE
Funding Support: This work was funded by the U.S. Department of Veterans Affairs, Veterans Health Administration, Office of Rural Health, NOMAD #PRFY-00614. The contents do not represent the views of the Department of Veterans Affairs or the United States government. This work was also funded by the University of Wisconsin Institute for Clinical and Translational Research, which is supported by the Clinical and Translational Science Award (CTSA) program, the National Center for Advancing Translational Sciences (NCATS), grant UL1TR002373 - KL2TR002374
Date of Acceptance: April 10, 2026 | Published Online Date: April 16, 2026
Abbreviations: CAT=COPD Assessment Test; CI=confidence interval; COPD=chronic obstructive pulmonary disease; COPD CARE=COPD Coordinated Access to Reduce Exacerbations; GERD=gastroesophageal reflux disease; GOLD=Global initiative for chronic Obstructive Lung Disease; QI=quality improvement; SD=standard deviation; VA=Veterans Affairs
Citation: Portillo EC, Do S, Hetzel S, et al. Symptomatic changes associated with a pharmacist-led COPD program. Chronic Obstr Pulm Dis. 2026; 13(3): 255-261. doi: http://doi.org/10.15326/jcopdf.2025.0716
Online Supplemental Material: Read Online Supplemental Material (167KB)
Introduction
Chronic obstructive pulmonary disease (COPD) symptoms are debilitating, persistent, and impact quality of life. Ability to work, social interactions, sleep, finances, and independence are affected by uncontrolled COPD symptoms.1,2 Despite evidence demonstrating how COPD symptoms can be improved through evidence-based practices and interventions, only one-third of patients receive the requisite level of care.1-3 Pharmacists are well-positioned to provide evidence-based practices and interventions to address care gaps and improve patient COPD symptoms.4 Unfortunately, there are few examples of care models where pharmacists deliver evidence-based care and interventions for COPD.5
Within the Veterans Affairs (VA) health system, pharmacists operate under a broad scope of practice that includes prescribing authority, allowing pharmacists to initiate, modify, or discontinue medications. COPD Coordinated Access to Reduce Exacerbations (COPD CARE) is a nationally scaled program that integrates pharmacists in VA primary care clinics as prescribers for COPD management.6 Pharmacists delivering COPD CARE within the VA provide critical interventions including adherence and inhaler technique reviews, symptomatic review, placement of referrals for pulmonary rehabilitation, COPD action plan development, medication optimization, and tobacco cessation support.
This evaluation explored the association between COPD CARE delivery and patient symptomatic changes. The primary outcome measured longitudinal changes in COPD symptoms. The secondary outcome investigated the association between specific interventions and symptomatic improvement.
Methods
Site Description
This retrospective cohort evaluation occurred within the Veterans Health Administration, which is the largest integrated health care system in the United States. Metrics detailing COPD CARE delivery were extracted from 28 Veterans Affairs medical centers located across the Midwest, Northeast, Southwest, and West regions of the United States.
COPD Coordinated Access to Reduce Exacerbations Program
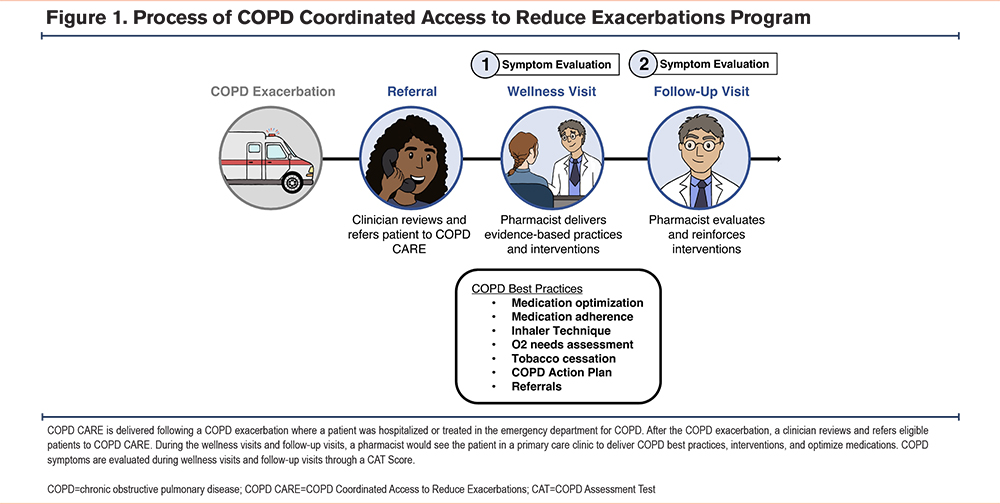
Patients were referred to COPD CARE following a recent hospitalization from an exacerbation. The program has been previously described in Portillo et al and Figure 1 shows how a patient progresses through COPD CARE.6,7 Referred patients received an initial wellness visit where pharmacists provided evidence-based practices and interventions. Pharmacists documented the following COPD-related interventions using a standardized note template provided during program implementation: identifying incorrect adherence and inhaler technique, referral to a service to support COPD management, developing COPD action plans, and changing medications (see Table 1 in the online supplement for definitions). A follow-up visit occurred 1 to 3 months later, during which patients were re-evaluated. COPD symptoms were assessed by pharmacists during each visit using the COPD Assessment Test (CAT) scoring tool. The CAT score is a validated, quantitative tool that allows patients to report symptoms using a holistic approach, including measures of dyspnea, sleep, and mobility, among other domains.8 Remeasuring CAT scores allows the pharmacist to assess the effectiveness of interventions provided during the wellness visit and reinforce or provide additional interventions during the follow-up visit. At follow-up visits, patients were also asked to self-report whether overall symptoms improved, stayed the same, or worsened since the wellness visit.
Data Collection
Unique patients who were referred to COPD CARE, had an initial wellness visit within 90 days of hospitalization, and received 2 CAT scores that were included in the analysis. Program delivery metrics were retrospectively extracted between September 2020 to February 2024 from the VA Corporate Data Warehouse, which is a database used to improve health care quality and patient safety across the VA health system.9
This evaluation was conducted to inform COPD CARE delivery across the Department of Veterans Affairs and was deemed a quality improvement (QI) initiative using the University of Wisconsin-Madison Institutional Review Board’s “QI/Program Evaluation Self-Certification Tool.”
Outcomes
The primary outcome of interest was the change in COPD symptoms as measured by CAT score differences between patient visits. Clinically meaningful symptomatic improvement was defined, a priori, as a CAT score improvement of ≥ 2 points between visits based on prior studies.10,11 Patients’ self-described COPD symptom changes were measured as a secondary outcome.
Analysis
Paired Student’s t-tests were conducted to assess the statistical significance of the change in CAT scores between the wellness and follow-up visits. Chi-squared tests of independence were conducted to evaluate the associations between binary variables of receiving each of the 6 interventions per pharmacists’ templated notes (yes/no) and clinically meaningful symptomatic improvement (yes/no). All analyses were done using R for statistical computing version 4.1. All tests were 2-tailed and conducted at a significance level of α = 0.05.
Results
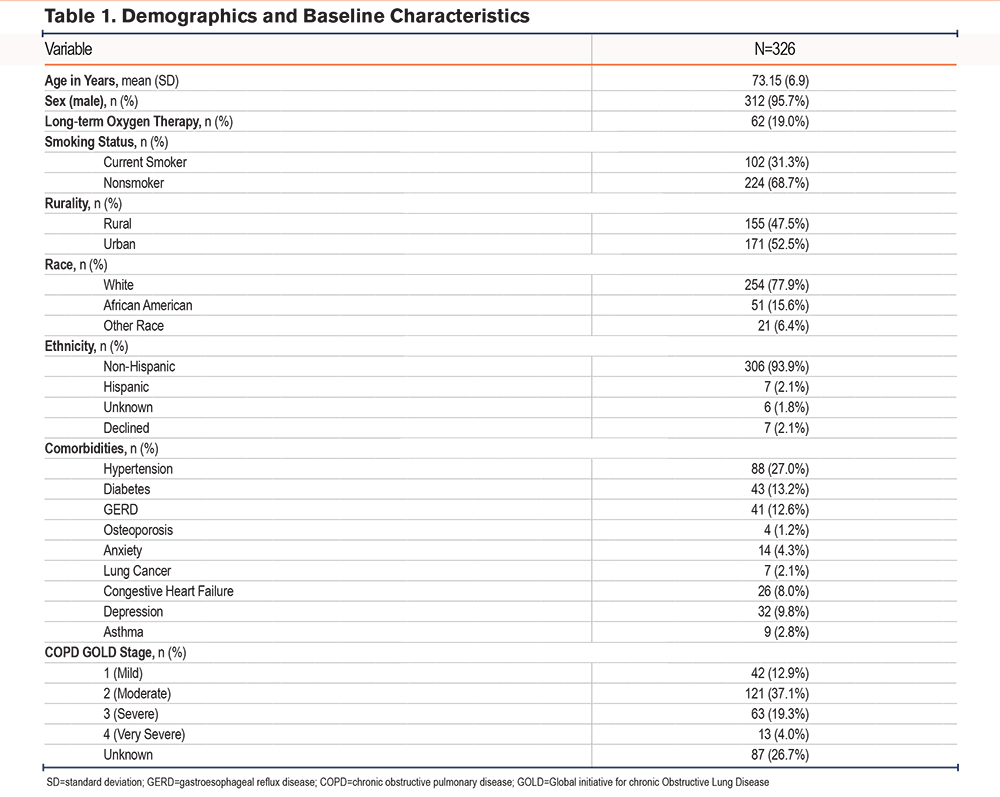
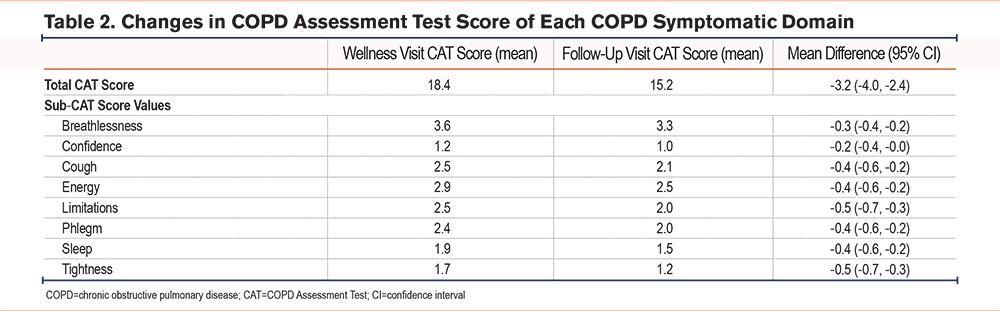
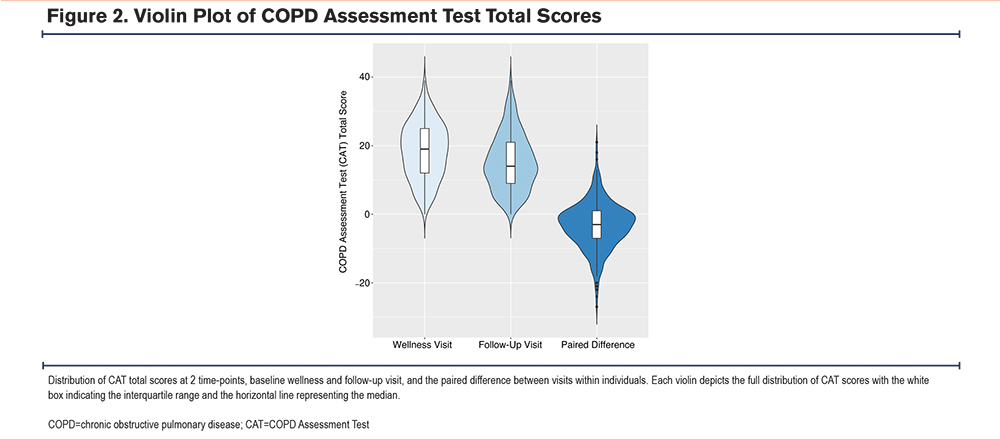
A total of 326 patients were included in the evaluation. Table 1 describes baseline characteristics of the patients in the evaluation. Between wellness and follow-up visits, a mean (standard deviation [SD]) CAT score improvement of 3.2 (6.8) points was observed (95% confidence interval [CI] 2.6, 4.0). Table 2 displays the mean difference in total CAT score as well as each CAT score component. The mean difference in total CAT score was both clinically meaningful and statistically significant, and statistically significant improvements were observed within each CAT score component. The distribution of CAT scores at the wellness and follow-up visits, as well as the distribution of paired differences between visits, are shown in Figure 2.
A total of 42 Veterans did not report whether symptoms changed (12.8%). Of those that did (N=286), 62.6% reported improved symptoms, 28.7% reported no change, and 8.7% reported worsening symptoms. Of note, patients who self-reported improved COPD symptoms experienced a mean (SD) CAT score improvement of 5.2 (6.0) points (95% CI 4.3, 6.1). Pharmacist interventions included identifying incorrect technique (N=62), changing medications (N=208), identifying nonadherence (N=117), providing service referrals (N=151), and developing COPD action plans (N=236). Patients receiving pharmacist-initiated medication changes experienced clinically meaningful symptom improvements (66.3%) significantly more often than those without medication changes (46.6%; p<0.001). No other interventions were significantly associated with clinically meaningful symptom improvement (see Table 1 in the online supplement).
Discussion
In this evaluation, the mean CAT score reduction of 3.2 points exceeded the 2-point threshold for clinical significance and supports the role of pharmacist involvement in COPD management programs. This real-world evaluation explores a comprehensive team-based care delivery model where pharmacists function as prescribers for COPD care transitions, contrasting with prior evaluations that have largely limited pharmacist roles to patient education. Mayzel et al evaluated a program where pharmacists corrected inhaler technique and nonadherence,12 but could not change therapies. Similarly, Bouwmeester et al evaluated the impact of pharmacist-led inhaler education,13 yet pharmacists did not have authority to optimize therapy as part of the service. While these and similar evaluations demonstrate promising outcomes,14-17 the impact of pharmacist-led care models with expanded clinical authority remains underexplored.
COPD CARE enables pharmacists to independently optimize patient therapy. Pharmacists in this evaluation provided a suite of interventions, including external service referrals, COPD action planning, and identification of incorrect inhaler technique. The integration of these evidence-based services likely contributes synergistically to symptomatic improvement. However, patients receiving pharmacist-initiated medication changes were more likely to experience clinically meaningful symptomatic improvement. This supports the value of pharmacists’ prescribing autonomy in managing complex chronic conditions. Importantly, this evaluation did not identify which medication classes or types of medication changes (e.g., discontinuation, initiation, dose adjustments) were most effective, presenting a valuable opportunity for future investigation on how to optimize clinical decision-making for patients with COPD.
This evaluation’s strengths include use of the validated CAT to capture a holistic measure of patient symptom burden and response to care. The national scale of COPD CARE provides evidence of program feasibility and effectiveness across a broad, diverse patient population. Unlike prior studies limited to a single institution,18-19 this evaluation spans across nearly one-fifth of the VA health care system, making it among the most widely scaled pharmacist-led COPD interventions to date. Our findings can inform future implementation and scaling of similar comprehensive COPD care programs.
However, this evaluation has limitations. Absence of a comparator group limits benchmarking opportunities across care delivery models. This analysis was retrospective, potentially introducing selection bias. To mitigate this, the use of within-subject paired analyses provided an internal control, enhancing confidence in the observed associations.
Our findings support pharmacist inclusion in multidisciplinary COPD care teams and underscore the need for structural changes to enable pharmacist billing mechanisms. Future research should explore integrating and reimbursing pharmacists within private sector primary care for COPD, as scaling beyond the VA system remains a challenge. Our findings also imply that pharmacist interventions may reduce readmission risk, given readmissions’ association with CAT scores.19 Efforts to explore this possibility are ongoing.
The VA has a capitated payment model and unique workflow which supports pharmacists in prescribing and comprehensive disease management roles.20 Differences in payment models could restrict scalability in the private sector, though value-based payment models that emphasize team-based, collaborative care presents an opportunity for pharmacists to deliver COPD management programs in non-VA primary care settings.21,22 Existing comprehensive COPD care models often rely on billable providers, such as nurses, physiotherapists, and physicians,23-26 and frequently exclude pharmacists.
In conclusion, this pharmacist-led COPD CARE program is associated with clinically meaningful reductions in patient symptom burden. These improvements appear to be driven by a combination of medication changes and integrated COPD interventions. This program offers valuable insights into the design and scale-up of team-based care approaches for COPD management, both within and beyond the VA system.
Acknowledgements
Author Contributions: ECP was the principle investigator and program innovator. SW was the national program manager. SW, MSM, and HO were responsible for the program implementation. MC was the supervisor. ECP was responsible for the funding. JVH was in charge of figure design and creation. ECP, SD, SG, PM, RSC, LD, DE, SW, MSM, and HO conceptualized and designed the evaluation. SH was responsible for the statistical data analysis. SD was in charge of data cleaning, PM was responsible for data extraction, CR tracked data decision making, and DE was in charge of data validation. ECP, JN, and KC wrote the original draft. ECP, SD, SH, JN, KC, CR, RSC, LD, MSM, HO, and MC reviewed and edited the manuscript. All authors approved the final manuscript to be published. All authors take responsibility for the integrity of the data and the accuracy of the analysis.
Disclaimer: The views expressed in this article are those of the authors and do not reflect the views of the United States Government, the Department of Veterans Affairs, or any of the authors affiliated academic institutions.
Declaration of Interests
All authors declare that they have no conflict of interests related to this evaluation.