Running Head: Small Vessel Volumes and Lower Oxygen in Smokers
Funding Support: Funding for this study was provided from National Institutes of Health, National Heart, Lung, and Blood Institute grants U01 HL089856 and U01 HL089897.
Date of Acceptance: April 10, 2026 | Published Online Date: April 16, 2026
Abbreviations: %LAA-950=percentage of low attenuation area below 950 Hounsfield units; 6MWD=6-minute walking distance; AVX=artery-vein phenotyping analysis; BMI=body mass index; BSA=body surface area; CI=confidence interval; COPD=chronic obstructive pulmonary disease; COPDGene=COPD Genetic Epidemiology study; CT=computed tomography; FEV1=forced expiratory volume in 1 second; FEV1 %pred=FEV1 percentage predicted; FVC=forced vital capacity; GOLD=Global initiative for chronic Obstructive Lung Disease, HU=Hounsfield units; IQR=interquartile range; mAgatston=modified Agatston; mMRC=modified Medical Research Council dyspnea scale; mPAP=mean pulmonary arterial pressure; OR=odds ratio; Pi10=square root wall area of an airway with a diameter of 10mm; PRISm=preserved ratio-impaired spirometry; SpO2=oxygen saturation assessed by pulse oximetry
Citation: Kwee AKAL, van Amsterdam WAC, Mohamed Hoesein FAA, et al. Small pulmonary artery and vein volumes independently predict oxygen desaturation in smokers. Chronic Obstr Pulm Dis. 2026; 13(3): 237-248. doi: http://doi.org/10.15326/jcopdf.2025.0694
Introduction
The pulmonary correlates of a decreased oxygen saturation in smokers are complex and multifactorial including airflow limitation, emphysema, ventilation-perfusion mismatch, cardiac dysfunction, and pulmonary vascular remodeling.1 In comparison to the extensive knowledge on the contribution of airways, alveoli, and perfusion in smoking-related lung disease, knowledge of the changes in smaller pulmonary vessels related to blood oxygen levels remains limited. This may in part be due to lack of quantitative methods for the in vivo measurement of the small pulmonary vessels. Fortunately, the advancement in artificial intelligence over the past years enabled automated quantification of small pulmonary vessels, small arteries, and/or small veins on computed tomography (CT).2-7
Recently, we investigated the role of small pulmonary arteries and veins determined from noncontrast CT scans obtained in the chronic obstructive pulmonary disease Genetic Epidemiology (COPDGene®) study and observed a higher mortality in participants with higher small pulmonary vein volume.8 Furthermore, we also found that both the number of pack years and smoking status were associated with higher small pulmonary vein and artery volumes.9 This raised interest in the role of small veins in smoking-related lung disease and we hypothesized that dilated veins could be related to a lower oxygen saturation independent of emphysema, airways, and heart disease. One of the possible explanations of dilated small pulmonary veins in smokers is based on findings from an established cast study,10 which described shunting between the bronchial veins (mostly oxygen poor) and pulmonary veins (mostly oxygen rich) in postmortem lungs with severe emphysema, potentially causing local hypoxemia. Shunting between bronchial arteries and pulmonary veins is another possibility. In addition to shunting there are several other theories, including venous dilation as a response to lower blood oxygen levels. Indeed, considering other organ systems, dilated retinal venules have been observed as a response to hypoxia and hypoperfusion,11,12 and it has also been suggested that hypoxia-induced factors are involved in the formation of varicose veins.13 Lower blood oxygen levels are also a common component in the pathophysiology of cardiac disorders such as heart failure or ischemic and hypertensive heart disease.14,15 In these patients, oxygen supply to cardiomyocytes is decreased due to microvascular obstruction and impaired vascularization. Additionally, a lower oxygen saturation could lead to venous wall thickening. For example, in residents with chronic hypoxia due to living at high altitude, medial hypertrophy of the pulmonary veins has been described in histological sections.16,17
As a next step in understanding the role of small veins disease in smokers’ lungs, we aimed to investigate whether, in individuals with a smoking history, a higher volume of the small pulmonary veins is associated with lower oxygen saturation and more frequent supplemental oxygen use.
Methods
Study Population
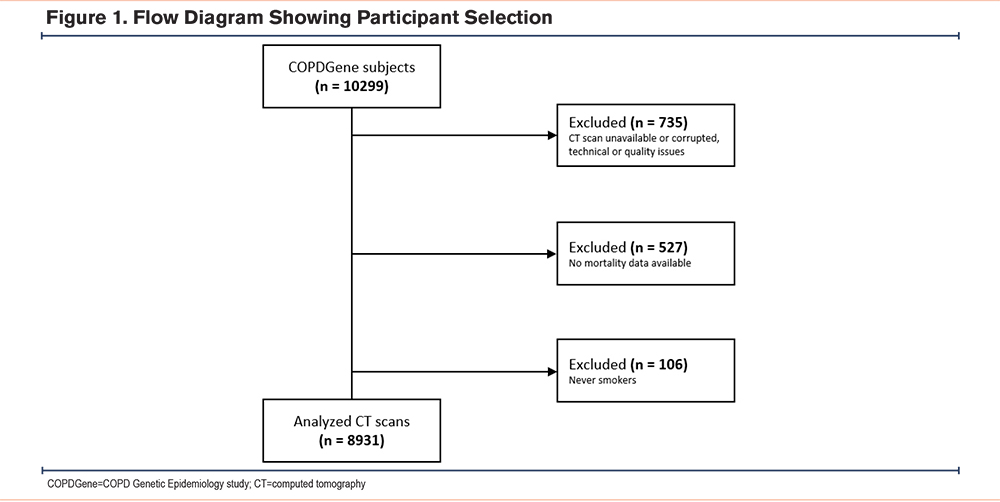
We included phase 1 participants of the COPDGene study (NCT00608764), in whom CT analysis was available (Figure 1). Data was collected18 in 2008–2011. All participants provided written informed consent. The full study protocol, including inclusion and exclusion criteria, was described previously.18
Spirometry and Clinical Data
Details on data collection are described in a previous paper.18 Spirometry data was measured postbronchodilator. Forced expiratory volume in 1 second (FEV1) and forced vital capacity are presented as a percentage of their predicted values.19 The pulmonary function test results were categorized according to the Global initiative for chronic Obstructive Lung Disease (GOLD) spirometry stages 0–4 or preserved ratio-impaired spirometry (PRISm).20
Race and pack years were self-reported with questionnaires. Body mass index (BMI) was calculated based on height and weight measurements. Functional exercise capacity was assessed with the 6-minute walking distance (6MWD). Activity-related dyspnea was self-reported with the modified Medical Research Council (mMRC) dyspnea scale.21
Oxygen Saturation
Oxygen saturation was measured after a resting position (seated) for >5 minutes, using a pulse oximeter on a finger without nail polish. In participants with supplemental oxygen use, the oxygen was discontinued during the saturation measurement. If oxygen saturation fell below 82%, the supplemental oxygen was restarted and a reading of 82% was registered.22
Computed Tomography Acquisition and Measurements
CT scan protocols have been described previously.18 Briefly, multidetector CT scanners (>16 detector channels) were used to acquire thin slice noncontrast-enhanced volumetric CT scans at inspiration (200mAs) and at the end of expiration (50mAs). Emphysema was calculated as the percentage of voxels below -950 Hounsfield units (HU) (%LAA950) on inspiratory CT scans. Emphysema was also visually assessed by expert readers according to the Fleischner Society and categorized as: none, trace, mild, moderate, confluent, or advanced destructive.23 Air trapping was quantified on expiratory CT scans and expressed as the percentage of voxels below -856 HU. Airway wall thickness was expressed as the square root wall area of an airway with a diameter of 10mm (Pi10).24 Coronary artery calcification was quantified with the modified Agatston (mAgatston) method, using the Agatston algorithm on ungated CT scans.25 All quantitative CT analyses were performed using Thirona’s lung quantification platform, LungQ® (Thirona; Nijmegen, The Netherlands).
Computed Tomography Pulmonary Vein and Artery Quantification
The pulmonary veins and arteries were quantified using the lung quantification platform LungQ®; details were published previously.8 In short, this method consists of 3 components: voxel-wise segmentation of pulmonary veins and arteries, separation of the identified vascular tree into individual branches, and quantification of vascular diameters and volumes for each branch.26-29 Small vein volume was quantified as the accumulated volume of all pulmonary venous branches with a diameter <1mm, and small artery volume as the accumulated volume of all pulmonary arterial branches with a diameter <1mm. To correct for inherent differences in body size, absolute small pulmonary venous and arterial were normalized by dividing it by body surface area (BSA), according to the DuBois method30 (BSA [m2]=0.007184 × Height [cm]0.725 × Weight [kg]0.425).
Statistical Analysis
All analyses were performed using R (version 4.3.3). Continuous variables were presented as mean ± standard deviation or median (interquartile range [IQR]). Missing values were present in 11 variables. In 9 variables (pack years, FEV1 percentage predicted [FEV1 %pred], emphysema, Pi10, resting oxygen saturation, mMRC dyspnea score, 6MWD, COPD GOLD stage, and CT scanner model), the percentage of missing values was <1%. In 2 variables (coronary calcium and visual emphysema severity), the percentages of missing data were 7.8% and 11.5%. All missing variables were imputed with multiple imputation. For imputation, the function “mice” was used from package mice (version 3.16.0). Data were imputed using 10 iterations, and 10 imputed datasets were generated.
Resting oxygen saturation was measured by pulse oximetry. Although the arterial oxygen tension relationship is nonlinear, most values in our cohort (>92%–99%) fell in the effectively linear upper portion of the curve, supporting the use of linear regression for association analyses. Logistic regression for categorical outcomes, such as oxygen-use, does not rely on this linearity assumption.
To investigate the association between resting oxygen saturation and small vein and small artery volumes, multiple linear regression was used, correcting for: age, gender, race, BMI, smoking status, pack years, FEV1 %pred, mMRC dyspnea score, 6MWD, %LAA950, Pi10, mAgatston score, severe exacerbations, supplemental oxygen use, pixel spacing, and scanner model. These covariates were selected a priori based on known associations with pulmonary vascular structure, hypoxemia, and CT-derived measurements, and to minimize confounding. Imaging and technical factors were included to account for variation in lung disease severity and acquisition-related measurement bias. Multivariable logistic regression was also used to analyze the association between supplemental oxygen use (yes/no) and small vein and small artery volume, corrected for: age, gender, race, BMI, smoking status, pack years, FEV1 %pred, mMRC dyspnea score, 6MWD, %LAA950, Pi10, mAgatston score, severe exacerbations, pixel spacing, and scanner model. Regression parameters are reported with their 95% confidence intervals. P values <0.05 were considered statistically significant.
Results
Participants' Characteristics
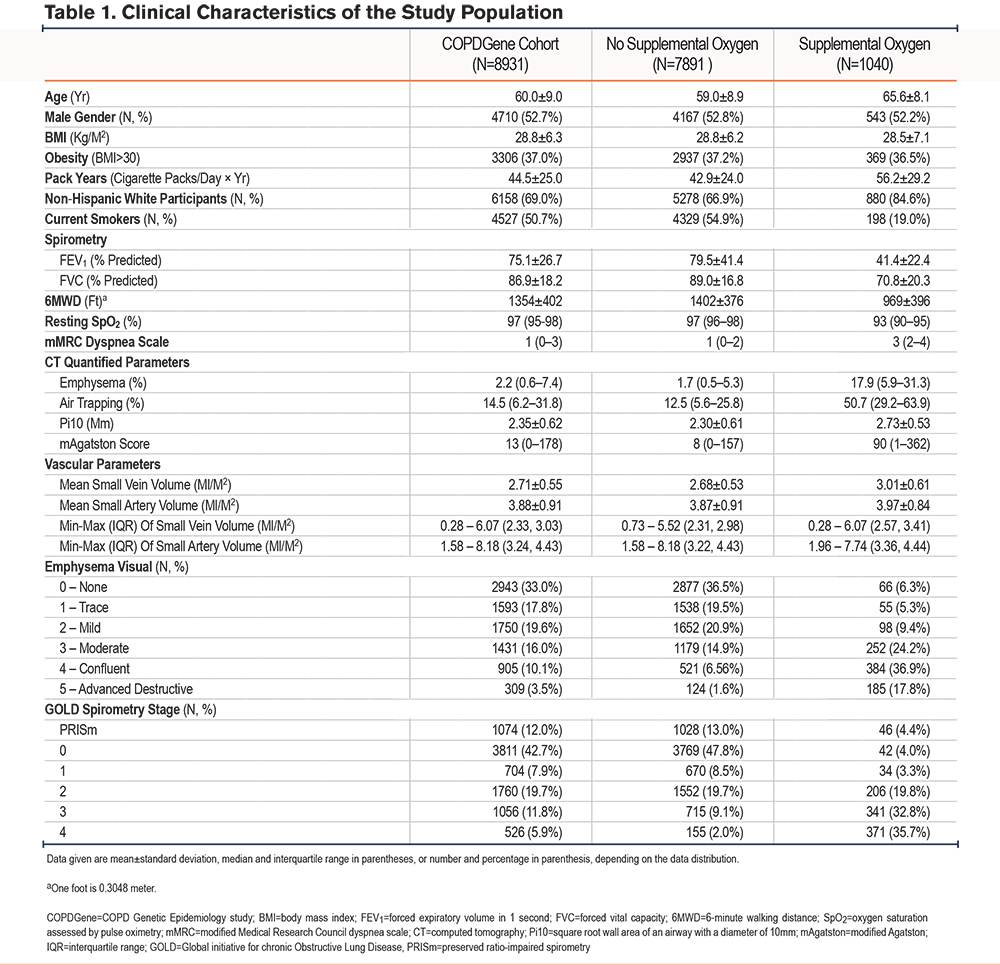
Of the 10,299 COPDGene participants who had completed phase 1, 735 were excluded because of corrupted or unavailable CT scans, 527 because of unavailable mortality data, and 106 because they were never smokers. Figure 1 shows a flow chart. The study population consisted of 8931 current and former COPDGene participants classified according to spirometry severity stages: 3811 GOLD 0, 1074 PRISm, 704 GOLD 1, 1760 GOLD 2, 1056 GOLD 3, and 526 GOLD 4. The average age was 60.0±9.0 years, and 52.7% were male. Among 4527 (50.7%) current smokers, there was a mean of 43.6±23.6 pack years smoked, while former smokers had a mean of 45.4±26.4 pack years. Median resting saturation was 97% (IQR 95%–98%), and 1040 (11.6%) participants used supplemental oxygen. Mean small vein volume was 2.71±0.55mL/m2. Mean small artery volume was 3.88 ± 0.91mL/m2. Further baseline characteristics are provided in Table 1.
Univariate Analysis
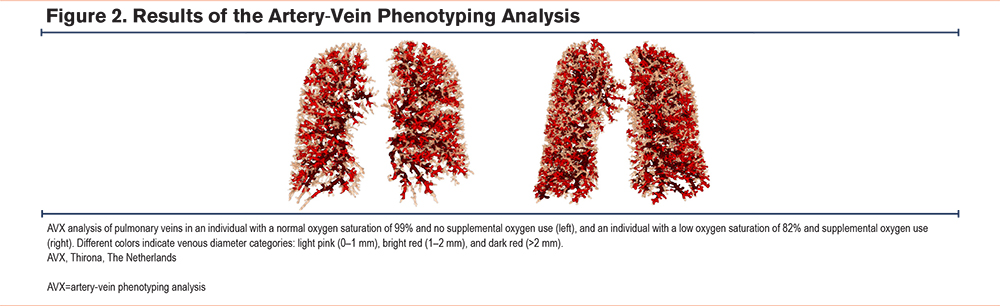
Of all participants, 1040 (11.6%) used supplemental oxygen. Univariable comparison (Table 1) showed that participants using supplemental oxygen were older (65.6±8.1 years versus 59.0±8.9 years) and had more pack years smoked (56.2±29.2 pack years versus 42.9±24.0 pack years). Supplemental oxygen users had more severe airflow obstruction, reflected by a lower FEV1 %pred (41.4%±22.4% versus 79.5%±41.4%) and higher amounts of emphysema (17.9% [5.9%–31.3%] versus 2.2% [0.6%–7.4%]), air trapping (50.7% [29.2%–63.9%] versus 12.5% [5.6%–25.8%]), and thicker airway walls (2.73±0.53mm versus 2.30±0.61mm). Mean small vein volume (3.01±0.61mL/m2) and mean small artery volume (3.97±0.84mL/m2) were higher in participants using supplemental oxygen compared to those without (2.68±0.53mL/m2 for veins and 3.87±0.91mL/m2 for arteries). See Figure 2 for representative 3D renders of pulmonary vein volume in participants from our population.
Multivariate Analysis
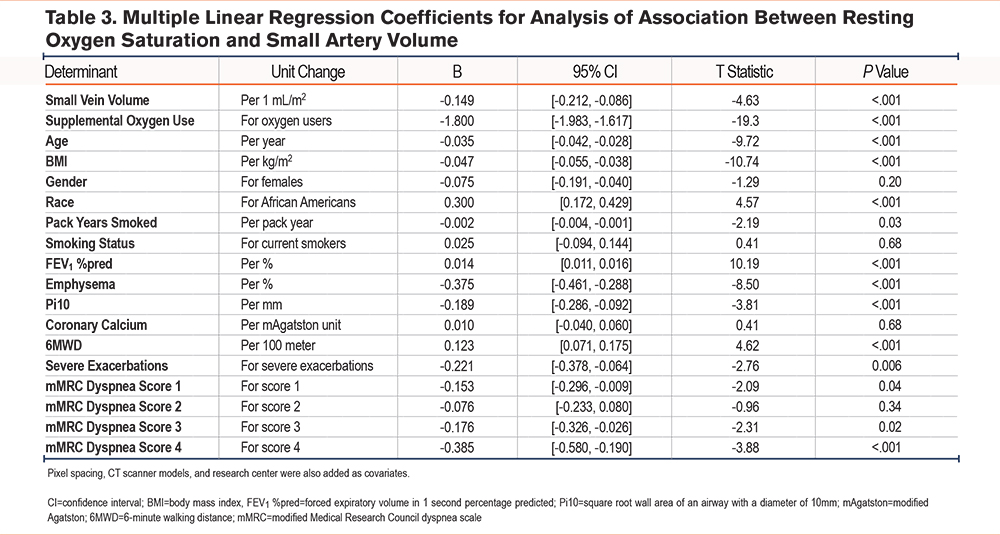
Multiple linear regression showed that for each 1mL/m2 greater small vein volume, oxygen saturation was 0.14% (0.25%, 0.03%) lower, after adjustment for other covariates (Table 2). For small artery volume, oxygen saturation was 0.15% (0.21%, 0.09%) lower (Table 3).

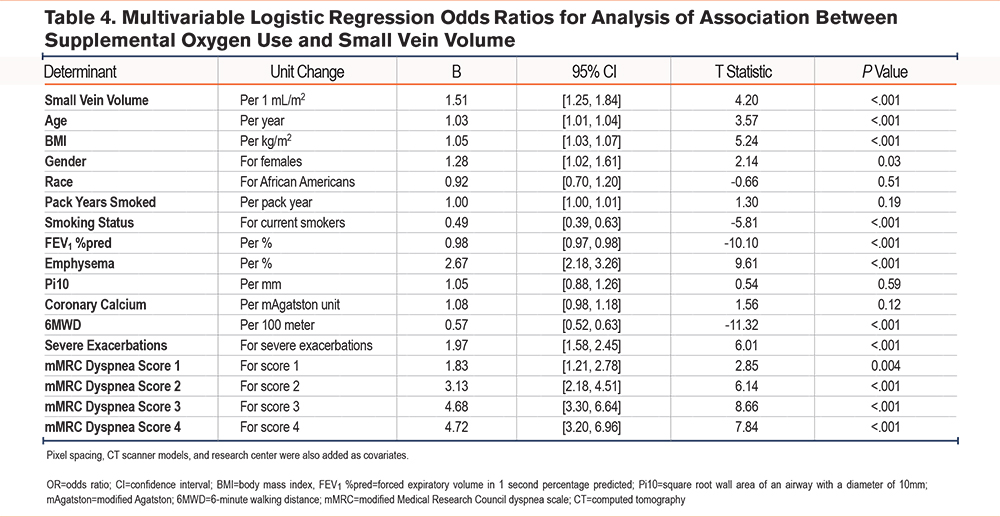
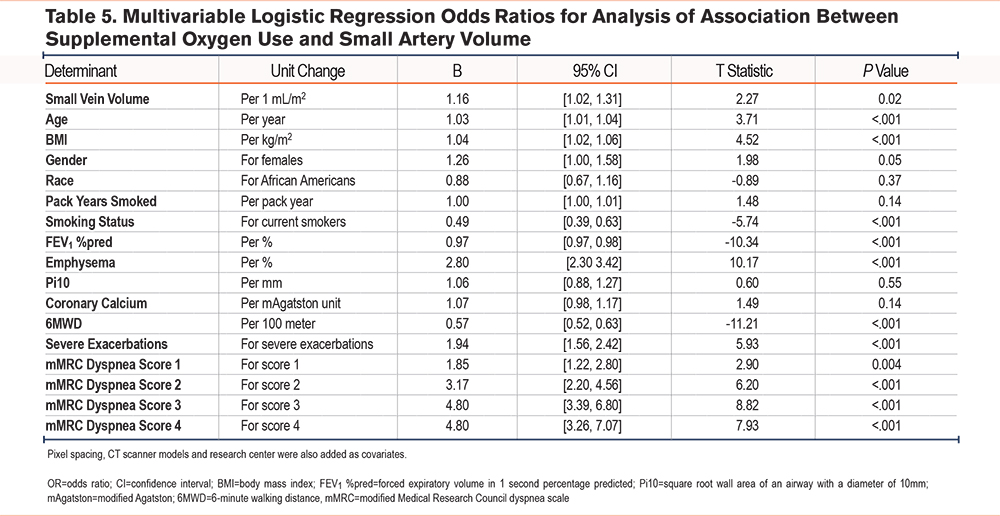
In multivariable logistic regression corrected for clinical and technical confounders, higher small vein volume (odds ratio [OR] per 1mL/m2 small vein volume 1.51 [1.25, 1.84]) and higher small artery volume (OR per 1mL/m2 small artery volume 1.16 [1.02, 1.31]) were associated with more frequent supplemental oxygen use. Results are shown in Tables 4 and 5.
Discussion
Our data showed that, in current and former smokers derived from the COPDGene cohort, higher volumes of small pulmonary veins and arteries are associated with a lower resting saturation and more use of supplemental oxygen when adjusted for various clinical and technical confounders. These results add to the growing interest in the relevance of the small pulmonary vessels, an understudied feature of the human lung.
Many studies have found that the pulmonary arteries constrict in response to alveolar hypoxia,31 but not much is known about the effect of oxygen levels on the pulmonary veins. In some pulmonary diseases where hypoxia is frequently present, including pulmonary veno-occlusive disease and pulmonary hypertension, remodeling and pruning of the small pulmonary veins has been described.32,33 Shelton et al measured venous wall thickness of postmortem lungs with emphysema and chronic bronchitis and found an increased wall thickness, especially in the smallest veins.34 Also, there is substantial evidence from animal studies that (chronic) low levels of oxygen have an effect on smooth muscle cells of the pulmonary veins, including hypertrophy and impaired contractility.35-37
We believe there are several possible explanations for our findings (Figure 3).
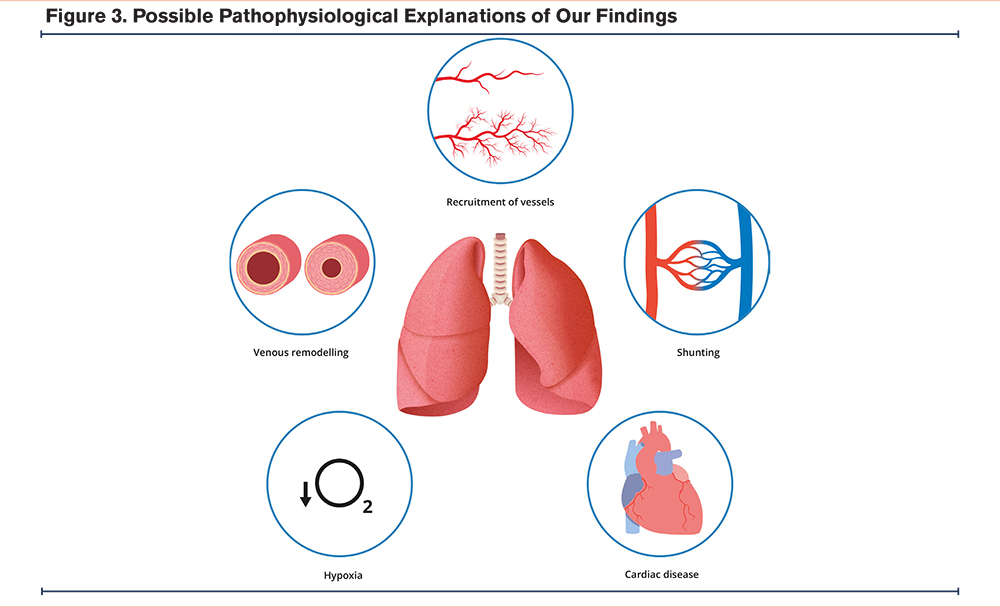
The first possibility is that there is a collateral circulation between the bronchial veins and the pulmonary veins, which has previously been described in severe emphysema established in a postmortem study.10 This would mean that blood from the bronchial veins (oxygen poor) mixes with the pulmonary veins (oxygen rich), leading to locally lower oxygen saturation and subsequent remodeling of the pulmonary veins.
Second, another related explanation is that direct shunts between the deoxygenated pulmonary arteries and the oxygen rich pulmonary veins occur, again leading to a decreased oxygen saturation. There is substantial anatomical evidence describing the existence of these arteriovenous shunts, including postmortem histological and cast studies in healthy lungs38-41 and also in vivo studies in COPD patients using wedge angiography.42,43 The etiology of these shunts is predominantly congenital, but have also been reported in acquired conditions such as hepatic cirrhosis, mitral stenosis, or trauma.44 In our cohort, no data is available on congenital conditions and no angiography has been performed.
Third, venous dilation could be a direct response to lower oxygen levels. Previous studies have described dilated retinal venules as a possible reaction to chronic retinal hypoxia or hypoperfusion.11,12 It has also been suggested that hypoxia-induced factors are involved in the formation of varicose veins.13,45 Consequently, intrapulmonary varicose veins could lead to lower oxygen levels through blood stasis. In this case, dilated veins would not be a cause, but a consequence of low oxygen saturation.
Fourth, the observed enlargement of venous and arterial volume could involve remodeling of the vessel wall, which has been found to occur in individuals with heart failure and pulmonary hypertension.46-48 The observed remodeling includes hypertrophy of the medial layer and elastic laminae. A study on explanted lungs found that intimal fibrosis and arterialization of the pulmonary veins frequently occurs in COPD.49 This remodeling could lead to an observed increase of small vein and artery volumes, when vessels that would normally be too small to measure are now detected as 0.2mm–1mm due to the thickened vessel wall.
Fifth, the higher small vein and artery volumes in individuals with lower oxygen levels could also be related to the recruitment of underused capillaries. There are a number of pulmonary capillaries at rest that are available “on demand” for the accommodation of an increase in blood flow, for example during exercise (West’s Lung Zone 2). These capillaries are recruited to keep the pulmonary pressure low in such situations.50-52 In the case of low oxygen saturation, as mentioned previously in the discussion, many studies have found that the pulmonary arteries constrict in response to alveolar hypoxia, leading to an increased pulmonary arterial pressure. To compensate for this increased pressure, there is a redistribution of blood flow to recruit underperfused capillaries, which helps to keep the pressure low and increases the surface area for gas exchange to compensate for the decrease in oxygen saturation.53 This recruitment can lead to not only an enlargement of the small vessels in previously underperfused areas (they need to accommodate for increased flow), but also tiny vessels that were not visible before can become visible due to enlargement. Additionally, at higher flows, there can be further distension of already perfused capillaries,50 accentuating this effect even more. In COPD patients, this “reservoir” of capillaries is already recruited at rest to compensate for the hypoxia induced by lung disease, meaning that there is no extra recruitment for increased flow due to exercise for example. This could also explain those COPD patients who have a normal mean pulmonary arterial pressure (mPAP) at rest but have an abnormally increased mPAP during exercise (exercise-induced pulmonary hypertension).
Lastly, low oxygen saturation is a common characteristic in many cardiac diseases including heart failure, ischemic heart disease, and hypertension. In these patients, chronic local hypoxia can be an effect of microvascular obstruction, impaired vascularization, and decreased oxygen supply to the heart.14,15 Microvascular dysfunction can, in turn, lead to stasis and accumulation of blood in the small veins and arteries, causing them to dilate. Furthermore, in mitral valve stenosis and pulmonary veno-occlusive disease an increase in pulmonary capillary pressures can lead to an increase in extracellular matrix.54 Unfortunately, we did not have specific cardiac measurements available to assess cardiac disease in our current cohort other than coronary calcium scores.
With this study, we want to emphasize that the lung is also a vascular organ and our data support further research into small pulmonary vessels. We can speculate that possible clinical implications of our findings include better phenotyping of lung diseases, specific drug therapy development aimed at the pulmonary vessels, or selecting specific pulmonary rehabilitation techniques.55
This study has several limitations. Due to the observational nature of our study, we cannot establish a causal relationship between oxygen levels and higher small pulmonary vein and artery volumes. A study with longitudinal follow-up measurements of vein and artery volume and oxygen saturation may strengthen the hypothesis of a causal effect if one measure would always precede the other. Second, oxygen saturation and vessel volumes were analyzed only at rest, as data during exertion, such as the 6MWT, were not available for all participants. Therefore, we have no information on the behavior of the vessel volumes as an immediate response to a decreased saturation. Investigating this in the future could give us more insight into the dynamic relationship of vein and artery volumes and oxygen levels.
Third, the unavailability of physiological and cardiac variables that could influence pulmonary vessel caliber (e.g., partial pressure of oxygen, arterial partial pressure of carbon dioxide, pH, B-type natriuretic peptide, troponin, hemoglobin, carboxyhemoglobin, pulmonary pressures, and sleep-disordered breathing), may have affected the observed relationship between oxygen saturation and small vessel volume. Fourth, clinical outcome data (e.g., mucus plugging or exacerbation history) and central vascular metrics such as the pulmonary artery to aortic diameter ratio were not consistently available in this dataset and therefore, we did not include these associations in our current analysis. Future studies are needed to explore potential relationships on how distal and central pulmonary vascular changes relate to each other and to clinically relevant outcomes. Additionally, we have no histological validation for our vascular findings. It remains a possibility that the observed enlargement includes not only vessel volume, but also surrounding tissue and extracellular matrix, such as interstitial fibrosis or lymph fluid. Also, the result of the software’s measurements has not yet been histologically validated, though adequate separation of the venous and arterial trees was visually confirmed.
Whether increased small vein and artery volumes are a cause or an effect of decreased oxygen saturation cannot be concluded from this study and a role for a cardiac cause remains a possibility. Further histological examinations of the small pulmonary vessels would be of interest, although intervention studies will be needed to ultimately unravel causality of the dimensions of small pulmonary vessels in the lungs of smokers and its relation to oxygen saturation.
In conclusion, higher volumes in the small pulmonary veins and arteries are associated with a lower resting oxygen saturation and more frequent supplemental oxygen use in smokers. These results highlight the relevance of the pulmonary vessels and urge further investigations into the small pulmonary vasculature.
Acknowledgements
Author contributions: AK, DL, SMH, PdJ, and EP conceived and conceptualized the study. DL, JC, and RC acquired the clinical data. JPC, LGE, and HT worked on development of the method and performing the quantitative CT analysis. AK and WvA performed statistical analysis. AK, LGE, JPC, FMH, PdJ, and EP wrote the manuscript. All authors contributed to data interpretation and revision of the manuscript. All authors read and approved the final manuscript.
Declaration of Interest
AK, WvA, FMH, and EP have no competing interests relevant to this manuscript. DAL, JC, SMH, and RC received grant support from the National Heart, Lung, and Blood Institute. PdJ declares that the Department of Radiology from the UMC Utrecht receives research support from Philips Healthcare. JPC is an employee and shareholder of Thirona. LGE and HT are employees of Thirona.