Running Head: Access to Virtual Pulmonary Rehabilitation
Funding Support: None
Date of Acceptance: April 22, 2026 | Published Online Date: May 11, 2026
Abbreviations: VPR=virtual pulmonary rehabilitation; PR=pulmonary rehabilitation; SVI=Social Vulnerability Index; SD=standard deviation; 1-MSTS=1-minute sit-to-stand test; CAT=COPD Assessment Test; mMRC=modified Medical Research Council dyspnea scale; PHQ-9=Patient Health Questionnaire-9; COPD=chronic obstructive pulmonary disease; IRB=institutional review board; EMR=electronic medical record
Citation: Schultz EA, Frank M, Eppler SL, et al. Who enrolls after referral to virtual pulmonary rehabilitation? A descriptive comparison. Chronic Obstr Pulm Dis. 2026; 13(4): 275-283. doi: http://doi.org/10.15326/jcopdf.2025.0729
Introduction
Chronic obstructive pulmonary disease (COPD) is a common pulmonary condition characterized by irreversible airway obstruction, exacerbations, and symptoms of shortness of breath, cough, and mucus production.1 In the United States, COPD is most commonly due to smoking, but other causes include long-term exposure to lung irritants like air pollution, as well as genetic conditions such as alpha-1 antitrypsin deficiency.2,3 COPD is the third most common cause of death globally. Approximately 24% of patients do not survive more than 5 years after diagnosis.4 Following diagnosis, patients with COPD report a reduced quality of life, physical inactivity, and functional decline.2 While pharmacotherapy treatment options exist for patients with COPD, multidisciplinary management, which combines pharmacotherapy, patient education, and pulmonary rehabilitation (PR), further improves outcomes for patients with COPD.5,6
PR combines pulmonary exercise training, patient education, and promoting behavior change to improve physical activity capacity.7 PR is one of the most effective treatments for patients with COPD, resulting in significant improvements in maximal exercise capacity, as well as patient-reported outcomes, including dyspnea, fatigue, and quality of life.8 PR has also been linked with decreased acute care utilization, including hospital readmissions, length of stay, and emergency department visits.9-11 Despite its innumerable benefits, PR remains grossly underutilized, with less than 5% of eligible patients participating in PR programs.12 Of those patients who do participate in PR, approximately 55% do not complete the program.13 There are multiple reasons for these low rates, one of which is a result of limited access to in-person PR programs. One study found that nearly 40% of Medicare patients had poor access to PR, with only one PR center within range for every 6030 individuals with COPD in the United States.14 Geographic limitations are one of the primary barriers to PR access, which is exacerbated by the increasing frequency of in-person center closures due to inadequate reimbursement. Other factors creating barriers to in-person PR access include existing medical comorbidities, a high volume of medical appointments, and transportation challenges.15,16 Therefore, one solution to overcome barriers in access to in-person PR may be virtual pulmonary rehabilitation (VPR).
VPR first emerged with the shift towards telemedicine amidst the COVID-19 pandemic.17 Several studies have found that at-home VPR programs were both feasible and effective in managing COPD, with significant improvements in the 6-minute walk test in patients using home-based PR.18,19 VPR is effective in improving additional patient outcomes such as health-related quality of life and functional performance.20,21 While there is some initial data suggesting VPR programs offer similar benefits to in-person PR, programs are heterogeneous, and there is limited evidence to support a more robust use of VPR programs. Additionally, there is very limited evidence available to demonstrate that VPR programs increase enrollment, improve patient access, and engage socially vulnerable populations. Therefore, the primary outcome of this study was to characterize the patients participating in a selected commercial VPR program (Kivo Health) as compared to referred but never-enrolled patients in terms of race, primary language, distance to the closest in-person PR program, and Social Vulnerability Index (SVI). Our secondary outcomes were to identify reasons patients declined to enroll in VPR and to assess the pre- and postprogram scores for functional capacity (1-minute sit-to-stand [1-MSTS] test), quality of life (COPD Assessment Test [CAT]), dyspnea severity (modified Medical Research Council Scale [mMRC]), and mood (Patient Health Questionnaire-9 [PHQ-9]) for patients across SVI groups.
Methods
In this retrospective study, we evaluated patients referred to a virtual PR program through a telehealth PR company (Kivo Health; San Francisco, California) from our institution between July 2023 and August 2025. This study was approved by Standford University Institutional Review Board (IRB-82136). Through a quality improvement project, our institution implemented a VPR program as an alternative to in-person PR to address access issues to in-person PR. After carefully vetting the commercial telehealth PR programs, Kivo Health was selected as the VPR provider and integrated into the electronic medical record (EMR) to facilitate a more streamlined referral process. Patients with COPD were then referred to Kivo Health primarily at the discretion of their referring pulmonologist.
Through the Kivo Health program, each participant completes an initial virtual one-on-one intake assessment to develop an individualized exercise regimen, incorporating moderate- to high-intensity aerobic activity with progressive advancement based on tolerance and performance. Group sessions are conducted by licensed respiratory therapists in cohorts of 2 to 5 participants via a secure, 2-way audiovisual telehealth platform. Physiologic monitoring is performed in real time using a wrist-worn pulse oximeter, enabling continuous assessment of heart rate and oxygen saturation throughout each session. Exercise intensity is evaluated through objective heart rate measurements and subjective ratings using the modified Borg scale. In addition to aerobic training, the intervention includes resistance exercises using elastic bands, as well as structured educational discussions on core topics in pulmonary rehabilitation. The program spans 8 weeks, with 2 sessions each week lasting approximately 90 minutes.
Cohort Selection and Outcomes
The VPR program cohort for our study included all patients referred by their provider to Kivo Health between July 2023 and August 2025. Demographic variables were collected for all patients participating in the VPR program using the EMR, including age, sex, zip code, race, and primary language. The patients’ zip code was used to calculate the average distance, in miles, to the nearest in-person PR center. Additionally, the zip code was used to calculate the SVI. The SVI was created by the Centers for Disease Control and Prevention and the Agency for Toxic Substances and Disease Registry and is a place-based index used to assess and quantify community-level social vulnerability.22 The SVI is created based on 16 Census variables measuring socioeconomic status, household characteristics, racial and ethnic minority status, and housing type and transportation.22 SVI values range from 0 to 1.0 and represent a percentile ranking, with higher values indicating higher social vulnerability. Scores are categorized as low (0 to 0.25), low to medium (0.26 to 0.50), medium to high (0.51 to 0.75), or high (0.76 to 1.0) vulnerability.23 Patients were categorized as either having completed the program, being active in the program at the time of data collection, or never enrolled in the program. Reasons for nonparticipation were collected for patients who declined enrollment following referral.
Patient outcomes included functional capacity (1-MSTS), quality of life (CAT), shortness of breath (mMRC), and mood (PHQ-9). The 1-MSTS test is used to assess exercise capacity in both in-person and virtual settings, measuring the patient's ability to sit and stand in a chair. A higher score on the 1-MSTS indicates decreased functional capacity.24 The CAT is a validated questionnaire that assesses COPD symptoms such as dyspnea, as well as measures of aerobic and functional capacity, and physical activity.25 The CAT is scored from 0 to 40, where a score of 0 indicates no health-related quality of life impairment, and a score of 40 indicates a severe impact on quality of life due to the disease.25 The mMRC is a 5-point scale from 0 to 4 based on the severity of dyspnea, with higher scores indicating more severe dyspnea.26 Finally, the PHQ-9 is a 9-item questionnaire used to determine the severity of depression, with higher scores indicating more severe depression.27 These outcome measures were recorded both before the start of the VPR program and following its completion. Data was provided to the investigators by Kivo Health under a data use agreement, and all analyses were performed independently by the investigators.
Statistical Analysis
Descriptive statistics were reported for all patients referred to Kivo Health VPR during the data collection period. Independent t-tests were used to compare age and average distance to in-person PR for active and completed patients with those who were never enrolled in VPR. Chi-square tests were used to assess statistical differences between groups for the categorical demographic variables. Paired t-tests were used to assess statistical significance between pre- and postprogram outcome measures. Statistical significance was set at α=0.05. R Studio was used for all analyses.28
Results
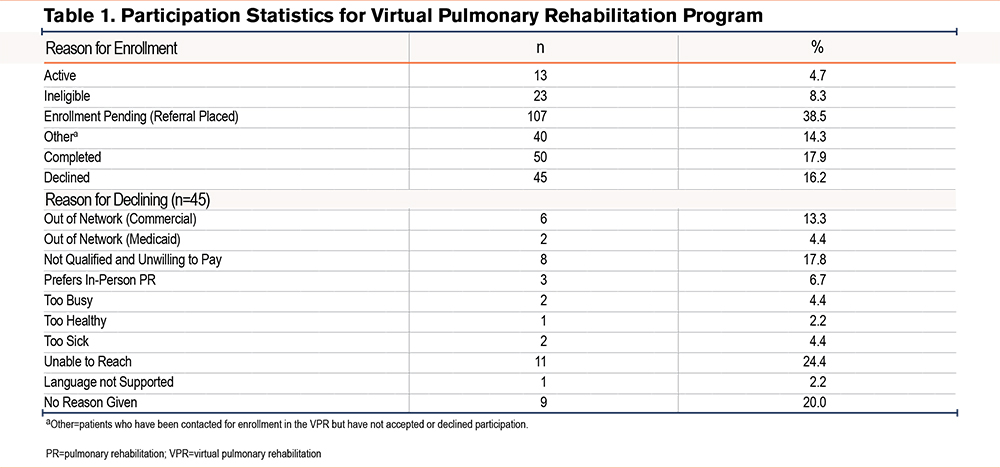
A total of 278 patients were referred to the Kivo Health VPR program between July 1, 2023, and August 31, 2025. Of the 278 patients, 63 (22.7%) had completed the VPR program or were active in the program at the time of data collection, with 50 (79.4%) having completed the program, and 13 (20.6%) being currently active in the program at the time of data collection (Table 1). Of the 45 patients who declined to enroll, most (11, 24.4%) were unreachable. Among the reasons patients reported for declining participation, the most common was that the program was out of network (8, 17.8%).
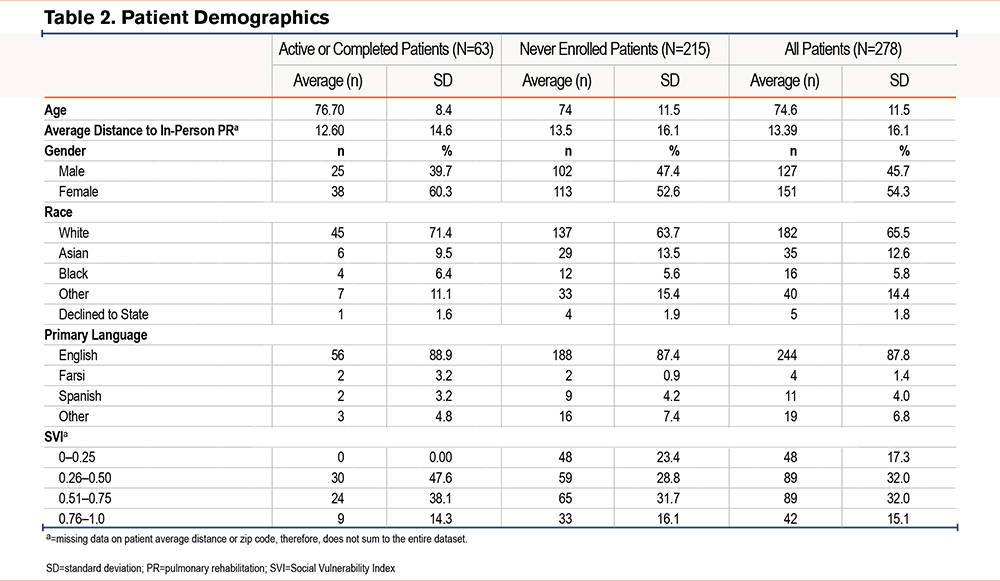
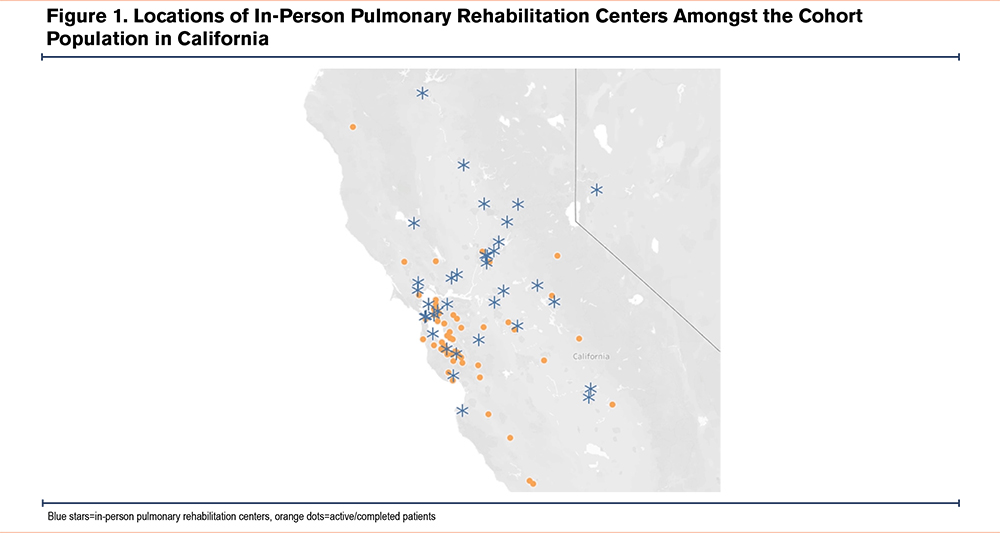
The average (standard deviation [SD]) age of the patients who were active in or completed the program was 76.7 (8.4) years of age, and most patients (40, 65.6%) were female, White (45, 73.8%), and their primary language was English (55, 90.2%) (Table 2). The average SVI for active/completed patients was 0.53 (range 0.36 to 0.97), with most patients (30, 46.9%) living in zip codes with low to medium social vulnerability. The average distance to an in-person PR center was 12.6 miles (range 0 to 67.1 miles) for active/completed patients, and there were 24 (37.5%) patients who lived more than 10 miles from an in-person PR center, and 14 (21.9%) who lived more than 20 miles from an in-person center (Figure 1). There were no statistically significant differences in demographic variables, including SVI, between participants who completed or were active in the VPR program and those who never enrolled (Table 2).
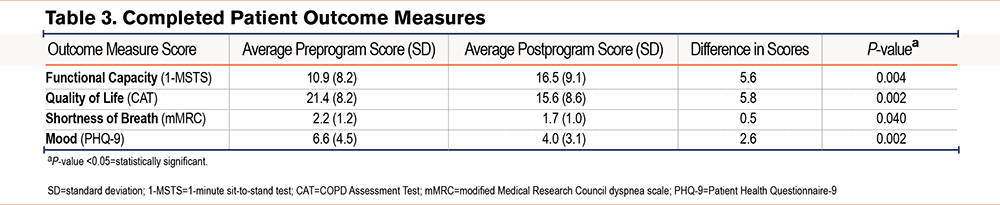
For patients who completed the program, the average (SD) preprogram 1-MSTS score was 10.9 (8.17), and the average postprogram score was 16.5 (9.1). The average preprogram CAT score was 21.4 (8.2) and the average postprogram score was 15.6 (8.6). The average preprogram mMRC score was 2.2 (1.2), and the average postprogram score was 1.7 (1.0). Finally, the average preprogram PHQ-9 score was 6.6 (4.5), and the average postprogram score was 4.0 (3.1). All measures demonstrated statistically significant improvements between pre- and postprogram scores (Table 3). There was only one adverse event reported in the cohort, which involved a fall sustained during the VPR program and did not result in additional workup or treatment.
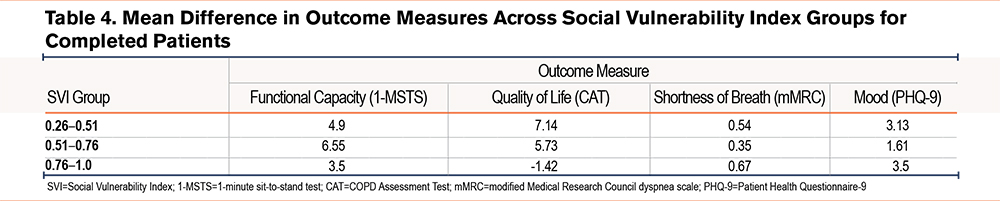
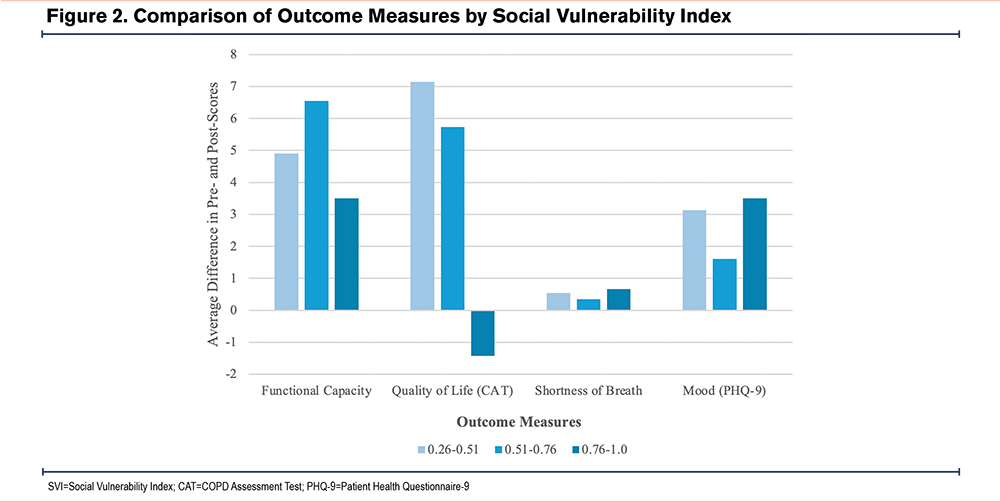
The mean difference in pre- and postprogram outcome measures was reported, with a subanalysis included based on patient SVI (Table 4, Figure 2). All measures demonstrated clinically positive improvements except for CAT scores in the high SVI (0.76–1.0) group. A posthoc Tukey test revealed significantly worse CAT scores in patients from the high SVI group compared to those from the low-medium SVI group (P=0.026).
Discussion
The development of VPR programs offers a promising strategy to overcome common barriers to accessing traditional PR services for patients with COPD. In our study, there were no significant differences in terms of patient characteristics between patients who participated in VPR and those who did not. Overall, VPR appeared to be accessible to patients across the range of SVI and distance from the nearest in-person PR, with statistically significant improvements in all outcome measures among VPR participants.
Despite the significant evidence of its effectiveness, one reason PR is underutilized is due to limited access. One of the main barriers to program uptake and completion is excessive distance to the nearest PR center. One study found that patients living over 10 miles from a PR program were half as likely to complete PR.29 In this study, we found that patients who participated in or completed VPR lived, on average, 12.6 miles from the nearest in-person PR program, and 22%, or more than 1/5 of patients, lived more than 20 miles from an in-person program. This suggests many of these patients may not have completed a PR program if VPR were not available.
However, excessive distance to the nearest PR center cannot explain why a significant portion of referred patients declined to enroll in a VPR program. Importantly, in this study for patients who were able to be contacted, lack of in-network insurance coverage was the most common reason for patients to decline participation, for both commercial and governmental insurance. So even though VPR may address geographic barriers to participation in PR, it appears that significant barriers to access to care due to insurance coverage are widening the care delivery gap for patients who would benefit from VPR. In addition to out-of-network insurance coverage, patients may differ in disease burden, functional status, or social drivers of health that are causing them to decline participation in VPR not captured in this study.30,31 Further research is needed to confirm these findings on a larger scale. These findings further underscore the need for continued advocacy to expand reimbursement for telehealth rehabilitation services for COPD patients.
In our study, it is also notable that there were no significant differences in demographics between the 215 patients who were referred to PR but had not enrolled at the time of data collection and those who were active in or had completed the program at the time of data collection. The majority of patients were White, in their 70s, female, and English-speaking, and were living in zip codes of medium social vulnerability. This primarily reflects the demographics of the population served by our institution. Low socioeconomic status tends to reduce the chances that patients will participate in and complete PR.32 However, there is a lack of studies investigating the role of specific social determinants of health measures, such as SVI, on patient participation in PR. A key finding is the absence of statistically significant differences in primary language, race, or SVI among patients. Although the diversity in our sample is low, this data suggests that socioeconomic vulnerability, race, and language are not the major barriers to enrollment in a VPR program.
SVI comprises many variables, including socioeconomic status, housing type, and transportation, all of which have been associated with decreasing access to PR. Therefore, VPR may be effective across SVI quartiles for patients of varying levels of social vulnerability. Although in-person programs may create barriers to completing PR, VPR may serve as a feasible option for patients with a range of social needs.
In addition, completion of the virtual program was associated with significant improvements in functional capacity, quality of life, dyspnea, and mood, underscoring its clinical benefit. These results align with previous studies that have investigated the role of similar VPR programs. For example, Filizola et al demonstrated high (88%) attendance and low rates (1%) of adverse outcomes for patients with COPD enrolled in a VPR program, with significant improvements in postintervention outcomes for the CAT, mMRC, 1-MSTS, and PHQ-9.33 Additional studies have investigated the role of a virtual-reality-based PR, which has similarly demonstrated improvements in dyspnea, lung function, exercise capacity, and oxygenation.34,35 Notably, in our study, all improvements in outcome measures were at or above the minimal clinically important difference, except for the PHQ-9 scores. This study further contributes to the evidence suggesting that VPR programs may offer tangible improvements in important outcomes for patients with COPD.
These benefits were observed across SVI, with patients in all SVI categories demonstrating improvements in outcomes, except for those with the highest SVI, who exhibited significantly worse CAT scores. It is unclear why patients in the high SVI group improved in all outcomes except for CAT scores, although CAT asks questions about energy, sleep, and confidence, which are not covered in the other patient-reported outcomes surveys and may be affected by other socioeconomic variables.
Limitations
This study is limited as these results are representative of only one cohort of patient referrals from a single academic institution and, therefore, may not capture all patients eligible for PR. However, this study aimed to include patients representative of the demographics at this institution and did not limit any patient demographics from enrollment in the study. Ideally, we aimed to compare patients referred to VPR with those referred to our institution’s in-person program during the same period to assess differences in demographics and outcomes. However, the in-person PR center had closed by the time of data collection, and the corresponding data were unavailable. Nonetheless, we believe the data presented remain valuable and allow for meaningful comparison with published literature to support our findings. It is noteworthy that pre- and postcomparisons are not available for a control group, which may limit causal inference. However, the clinical improvements reported in this cohort provide preliminary evidence of the benefits of a VPR program and may be further investigated in randomized controlled trials. In addition, the average distance to in-person PR centers is limited, as we were only able to track zip code-level data rather than granular patient and center addresses. However, we report these values as broad estimates to capture the estimated distance to in-person centers. SVI is a community-level measure which may not capture the social vulnerability of every individual, which may present risk of ecological fallacy when compared to individual clinical outcomes that were collected. However, community-level metrics were reported in this study as these metrics may improve the assessment of VPR programs across communities. Finally, referrals made to the VPR program were made at the discretion of referring physicians, which may contribute to a selection bias of patients who were deemed fit for the VPR program. However, we aimed to mitigate this risk given the larger sample size from a large academic center that sees a diverse patient population. We hope these findings will serve as a foundation for future multicenter studies involving larger and more diverse patient populations to further validate and expand upon the results presented in this study.
Conclusion
In this study, we demonstrated that VPR programs may increase access for geographically underserved and socially vulnerable populations, while still leading to clinically significant improvements in both objective and patient-reported outcomes. However, inadequate insurance coverage remains a key obstacle to VPR enrollment, and continued advocacy is essential to expand reimbursement for this service.
Acknowledgements
Author contributions: MD and MF had full access to the data in the study and take responsibility for the accuracy of the data. ES completed the data analysis and takes responsibility for the integrity of the data and the accuracy of the data analysis. ES, MF, SE, MD, RNK, JM, and LE contributed substantially to the study design, data analysis and interpretation, and the writing of the manuscript. LE takes responsibility for the content of the manuscript, including the data and analysis. All authors approved of the final version of the manuscript.
Declaration of Interest
The authors declare they have no competing interests.