Running Head: AATD Gene Therapy Knowledge and Perspectives
Funding Support: This is an unfunded study with questionnaire and administrative support provided by AlphaNet, Inc.
Date of Acceptance: May 21, 2026 | Published Online Date: June 1, 2026
Abbreviations: AAT=alpha-1 antitrypsin; AATD=alpha-1 antitrypsin deficiency; ADMAP=Alpha-1 Disease Management and Prevention; ANOVA=analysis of variance; CDC=Centers for Disease Control and Prevention; COPD=chronic obstructive pulmonary disease; FDA=U.S. Food and Drug Administration; GED=general education development; HSD=honestly significant difference; NIH=National Institutes of Health; REACH=Risk Evaluation to Achieve Continued Health
Citation: Foil KE, Stern MM, Strange C, et al. Gene therapy: knowledge, attitudes, and preferences among individuals with alpha-1 antitrypsin deficiency. Chronic Obstr Pulm Dis. 2026; 13(4): 293-304. doi: http://doi.org/10.15326/jcopdf.2026.0784
Online Supplemental Material: Read Online Supplemental Material (424KB)
Introduction
Alpha-1 antitrypsin deficiency (AATD) is caused by pathogenic variants of the SERPINA1 gene that encodes the circulating serine protease inhibitor alpha-1 antitrypsin (AAT).1 When insufficient levels of AAT reach the lungs, unchecked protease activity leads to progressive lung damage and the eventual onset of chronic obstructive pulmonary disease (COPD).2,3 The liver is the main site of AAT production, and liver disease can result when the accumulation of a misfolded form of AAT in hepatocytes triggers an exaggerated inflammatory response.4-6
AATD affects at least 1 in 2500 individuals in the United States and follows an autosomal codominant pattern of inheritance.6 SERPINA1 alleles that code for normal AAT are generally designated “M.” Allelic combinations that include 1 or 2 non-M alleles may result in low AAT levels and cause increased risk for COPD and liver cirrhosis. The most common AATD-associated alleles are known as “Z” (c.1096G>A; p.Glu366Lys; ClinVar Variation ID 17967) and “S” (c.863A>T; p.Glu288Val; ClinVar Variation ID 17969), and the Z allele encodes a misfolded form of AAT that forms polymers that accumulate in hepatocytes. Individuals who are homozygous for this variant (ZZ) typically have severely deficient AAT serum concentrations.7,8 The S variant typically results in a moderate AAT deficiency without polymerization and associated risk for liver disease, and numerous other pathogenic variants affect AAT quantity, function, or both.
The management of AATD lung disease includes standard COPD therapies, as well as, for many, the use of augmentation therapy, which is an AATD-specific treatment requiring regular intravenous infusions of plasma-derived AAT.9-12 While augmentation therapy does not reverse lung damage, it does delay emphysema progression.13 There is currently no approved, specific treatment for AATD-associated liver disease other than liver transplantation, which is typically reserved for those with the most severe cirrhosis.14 While liver transplantation is generally successful in relieving both the liver and future lung phenotypes of AATD, its complexity, limited organ availability, and issues related to immune suppression limit the feasibility of wider implementation.
Given the limitations of available treatments, gene therapy holds great promise for the treatment of AATD. A therapy capable of driving the delivery of sufficient levels of AAT to the lungs could prevent the onset or progression of lung disease, and one capable of preventing the accumulation of misfolded AAT in hepatocytes could prevent the onset or progression of liver disease. Such gene therapies are already under development and in clinical trials, and many are discussed in a recent review.15 These treatments include some that target either the lung or liver problem independently and others that target both simultaneously. Such variety is useful given the different pathogeneses of lung and liver disease in AATD.
Patient knowledge and perceptions of gene therapies are likely to inform attitudes and preferences towards gene therapies and ultimately influence the likelihood of choosing to receive a particular gene therapy or participate in a particular gene therapy clinical trial.16-23 Research across populations of patients with different genetic conditions has demonstrated that patients have limited knowledge of how gene therapies work, including frequent misunderstanding of benefits, limitations, risks, and implications of receiving a gene therapy or participating in a gene therapy clinical trial.16-18,24-29 Understanding patient knowledge, attitudes, and preferences regarding gene therapies is essential for ensuring therapies are aligned with patient preferences and meet patient expectations. Improved understanding of patient preferences can also inform components of adequate education and improve the informed consent process.
No prior studies have investigated the knowledge, attitudes, and preferences of individuals with AATD regarding gene therapies or gene therapy clinical trials. The purpose of this study was to fill this gap using a research instrument designed to assess knowledge related to gene therapy for AATD, attitudes towards gene therapy and gene therapy clinical trials, and the impact of different characteristics of a hypothetical gene therapy clinical trial on the likelihood of participating. The results of our study can be used to inform clinical trial design, identify potential misconceptions, and fill knowledge gaps so that patients are appropriately informed and empowered when making gene therapy decisions.
Methods
Study Design
An electronic invitation to participate in this survey-based study was sent to 4552 individuals enrolled in AlphaNet, a not-for-profit disease management organization. Study inclusion criteria were: (1) age >18 years, (2) AATD, (3) consent to use the data for research, and (4) access to the AlphaNet portal with email. Data were collected between September 24, 2024, and November 15, 2024. The study was approved by the Western Institutional Review Board-Copernicus Group (study number 1349750).
Individuals with AATD provided input into development and refinement of the data collection instrument; these individuals were ineligible to participate in the study to minimize the potential for bias. Knowledge related to AATD gene therapy was assessed using 12 multiple-choice questions representing 4 different gene-related knowledge domains. Attitudes and preferences towards gene therapy were assessed using Likert-scale items. Open-ended short response questions were also included. Demographic information collected included self-reported age, sex, race, and highest level of education completed. Health information collected included time since AATD diagnosis, AATD genotype, presence of lung and/or liver disease and number of hospitalizations for each, number of pulmonary exacerbations in the past year, current supplemental oxygen use status, and number of AATD-related conferences or learning days attended. The complete research instrument and details of its development are included in the online supplement.
Data Analysis
Surveys were included if participants completed a predefined minimum set of key variables (demographics and at least one primary outcome domain related to knowledge, attitudes, or preferences). Partial responses were retained to maximize data use, and analyses were conducted using available data for each item (i.e., pairwise deletion). Quantitative data were analyzed using JMP® Pro 18.0.2 (JMP; Cary, North Carolina). Interactions between specific demographic or health characteristics and knowledge were analyzed by identifying clinically or demographically relevant groups and then comparing the average number of correct responses between groups using either one-way analysis of variance with Tukey-Kramer honestly significant difference (HSD) posthoc analysis or t-test. The number of knowledge assessment questions answered correctly was used to divide the population at the median for comparative analyses of differences in mean numerically-converted Likert-scale responses to attitude and preference items using t-tests. P values<0.05 were accepted as significant for all quantitative analyses. Responses to open-ended questions were analyzed using thematic analysis, following an iterative coding process by 2 researchers. Additional methodological detail is described in the online supplement.
Results
Characteristics of the Study Population
Of the 4452 individuals invited, 1112 (25% response rate) completed all or part of the survey. The demographic and health characteristics of participants are summarized in Table 1. Over half of participants (55%) were age 65 or older, 56% were female, and 98% were White, non-Hispanic. Approximately 40% of participants had attended at least one AATD conference or learning day, with 29% having attended 2 or more.
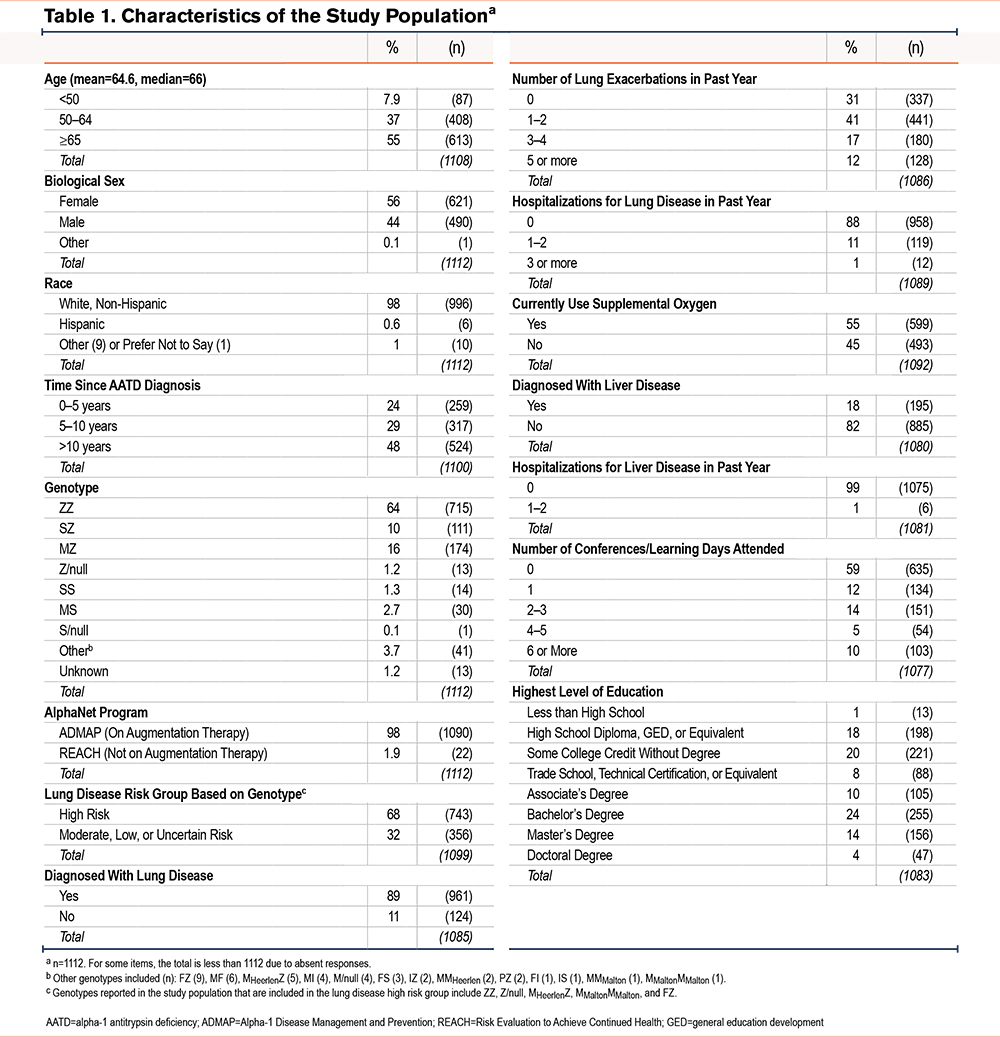
Nearly half of the participants (48%) received their diagnosis of AATD 10 or more years ago, and less than 23% reported their diagnosis for less than 5 years. The most common genotypes reported were ZZ (64%), MZ (16%), and SZ (10%) with no other genotype surpassing 3% of the study population. Over two-thirds (68%) of participants reported having a genotype associated with severe AAT deficiency. Nearly 90% of participants had been diagnosed with lung disease, and 55% were using supplemental oxygen. Among the 69% who had at least one pulmonary exacerbation in the past year, 12% required hospitalization. Less than 20% of participants had been diagnosed with liver disease with only 1% requiring hospitalization for their liver disease within the past year.
Participant Knowledge Related to Gene Therapy for Alpha-1 Antitrypsin Deficiency
Twelve knowledge questions assessed 4 knowledge domains: (1) genes and gene expression, (2) gene therapies, (3) clinical trials, and (4) AATD etiology and genetics. Each question had answers characterized as correct or incorrect, and participants could select an answer option of “unsure.” A summary of the percentage of correct, unsure, and incorrect responses for each knowledge domain and each question is provided in Figure 1A. A brief and simplified representation of the specific knowledge being assessed for each question is included.
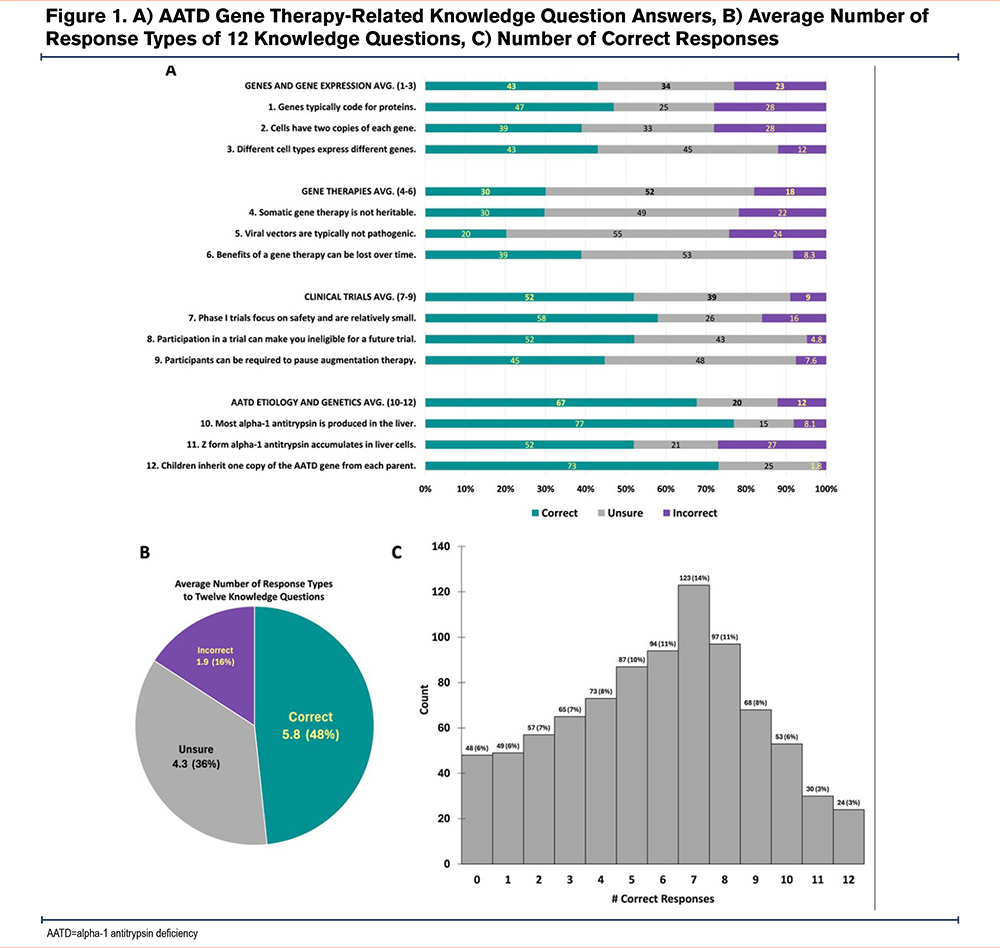
The correct response rate was highest for the domain of AATD etiology and genetics (67%) followed by the domains of clinical trials (52%), genes and gene expression (43%), and gene therapies (30%). The unsure response rate was highest for the domain of gene therapies (52%), followed by clinical trials (39%), genes and gene expression (34%), and AATD etiology and genetics (20%). The incorrect response rate was highest for the domain of genes and gene expression (23%), followed by gene therapies (18%), AATD etiology and genetics (12%), and clinical trials (9%).
On average, participants answered 5.8/12 (48%) questions correctly, answered unsure for 4.3/12 (36%) questions, and answered 1.9/12 (16%) questions incorrectly (Figure 1B). The median number of correct responses was 6/12 (range 0–12). Figure 1C shows the distribution of the number of correct responses across the study population. For subsequent analyses of the interaction between knowledge and attitudes or preferences, participants who answered all questions were divided into 2 groups: (1) those who answered 6 or more questions correctly (median or above, 56% of participants); and (2) those who answered 5 or fewer questions correctly (below median, 44% of participants).
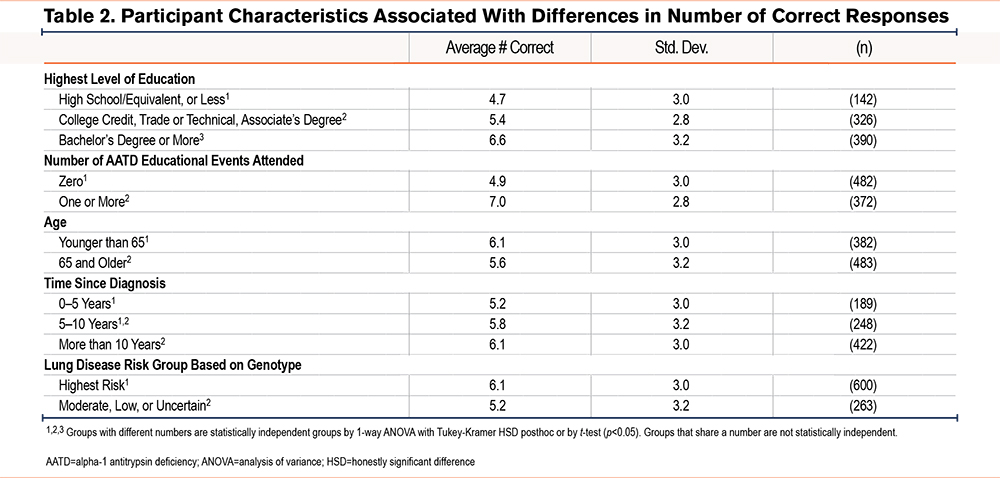
We also evaluated whether differences in demographic and health characteristics were associated with differences in knowledge. Higher level of education, attendance of AATD educational event(s), age <65, increased time since diagnosis, and high genetic risk for lung disease correlated with higher knowledge scores (Table 2).
Responses to open-ended questions asking about gene therapy information needs and potential sources are summarized in Supplemental Tables 1 and 2 in the online supplement. The 5 most common response themes for desired additional information were: (1) general desire for more information (included in 24% of responses); (2) safety, risks, side effects, and/or limitations (23%); (3) efficacy and expected benefits (17%); (4) the results of gene therapy research and clinical trials (13%); and (5) details of how gene therapy is administered and the logistics associated with receiving a gene therapy or participating in a clinical trial (13%). Notably, 4% of responses indicated that no additional information was desired. The 5 most commonly listed trusted information sources were the Alpha-1 Foundation, AlphaNet, and/or the alpha-1 community (included in 63% of responses), doctor(s) or other health care providers involved in participants’ AATD care (28%), the internet (10%), scientific literature/research (7%), and government agencies (including the National Institutes for Health, U.S. Food and Drug Administration [FDA], Centers for Disease Control and Prevention, and ClinicalTrials.gov), and the nonprofit National Organization for Rare Disorders (5%). Notably, 9% of the responses indicated uncertainty in where to seek information about gene therapy.
Participant Attitudes Towards Gene Therapy
Figure 2 includes a brief and simplified representation of each item used to assess participant attitudes related to gene therapy along with the distribution of responses. The percentage of respondents who replied “somewhat high” or “very high” increased when moving from willingness to participate in a non-gene therapy clinical trial (40%) to a gene therapy clinical trial (48%) and further increased for an FDA-approved gene therapy (65%). Similarly, concern for the safety of gene therapy clinical trials (44% somewhat/very high) was greater than concern for the safety of FDA-approved gene therapies (39% somewhat/very high).
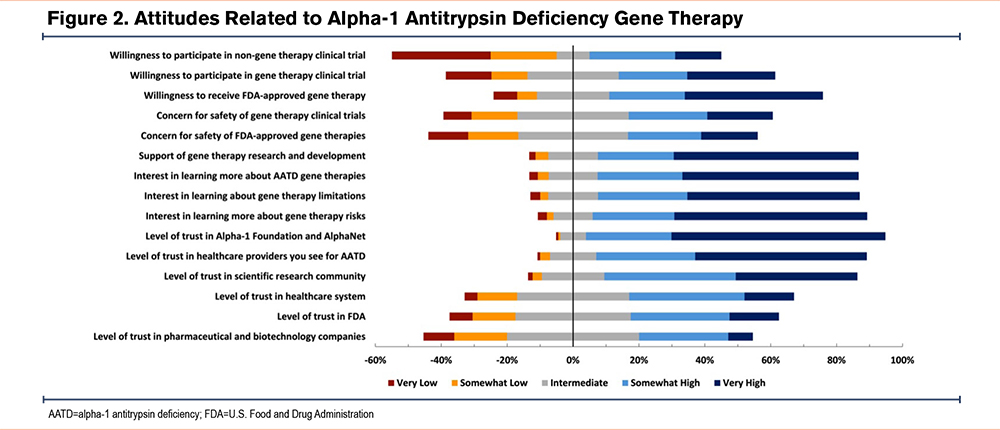
Participants expressed high levels of interest in learning more about AATD gene therapies (80% somewhat/very high) and support of gene therapy research and development (79% somewhat/very high) as well as high levels of interest in learning more about gene therapy risks (84% somewhat/very high) and limitations (79% somewhat/very high). Participants expressed the highest levels of trust in the Alpha-1 Foundation/AlphaNet (91%) followed by their AATD health care providers (82%), the scientific research community (77%), the health care system (50%), the FDA (45%), and pharmaceutical/biotech companies (35%).
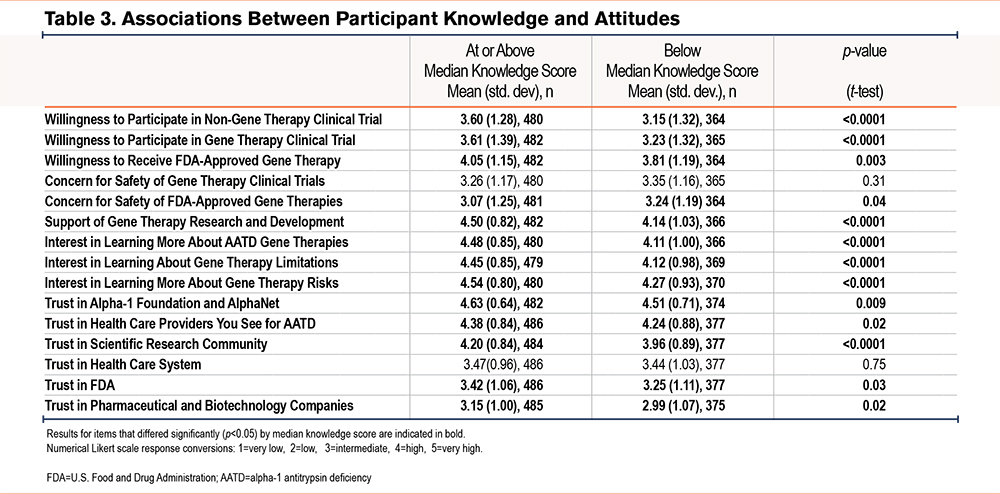
To determine if participant knowledge is associated with differences in attitudes towards gene therapy, mean numerical Likert scale responses were compared between respondents who answered 6 or more knowledge questions correctly (those at or above the median) and those who answered 5 questions or fewer correctly (those below the median) (Table 3). Higher knowledge correlated with more favorable attitudes for all but 3 items: there was no difference in concern for safety of gene therapy clinical trials or level of trust in the health care system between groups, and the below median knowledge score group had higher concern for the safety of FDA-approved gene therapies.
Participant Preferences in Gene Therapy Clinical Trial Characteristics
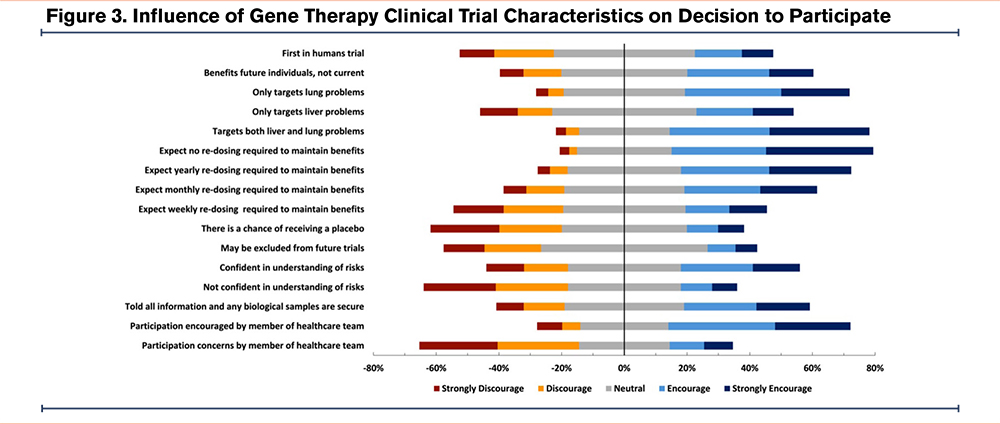
To assess preferences, participants were asked whether several characteristics of a hypothetical gene therapy clinical trial would discourage or encourage their likelihood of participating. Figure 3 includes a brief and simplified representation of each characteristic and shows the distribution of responses for each item. Based on the percentage of encourage/strongly encourage responses, characteristics that most encouraged participation were: use of a single dose of gene therapy expected to maintain benefits (64%), and a therapy targeting both lung and liver problems (64%). Based on the percentage of discourage/strongly discourage responses, characteristics that most discouraged participation were the participant’s care team member expressing concerns about participation (51%), not being confident in understanding the risks associated with the gene therapy (46%), chance of receiving a placebo (42%), expectation of weekly re-dosing to maintain benefits of the gene therapy (35%), and the possibility of being excluded from future gene therapy clinical trials (31%).
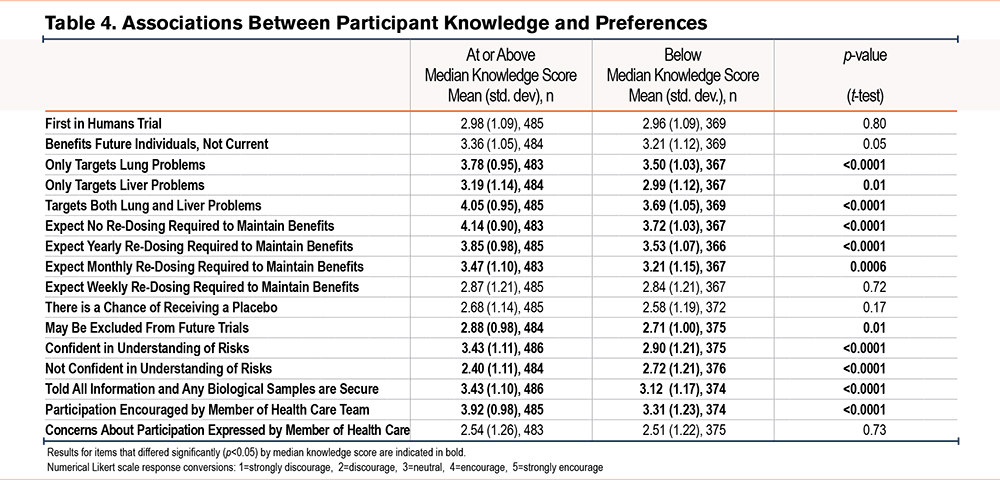
To determine if participant knowledge was associated with differences in clinical trial preferences, mean numerical Likert scale responses were compared between respondents at or above median knowledge to those below (Table 4). The mean numerical Likert scale response was higher (characteristics were more encouraging or less discouraging) in the higher knowledge score group for 10/16 items. In addition, the at or higher knowledge group was more discouraged if not confident in understanding of risks.
Participant responses to open-ended questions asking about factors that would most increase or decrease the likelihood of participating in an AATD gene therapy clinical trial are summarized in Supplemental Tables 3 and 4 in the online supplement. The 5 most common factors found to increase the likelihood of trial participation were a low burden of participation (included in 30% of responses), having additional information/knowledge about gene therapy (20%), evidence of efficacy (14%), the ability to continue augmentation therapy and other treatments during the trial (8%), and evidence of safety (8%). The 5 most common factors found to decrease likelihood of trial participation were a high burden of participation (included in 33% of responses), safety concerns (25%), having to pause augmentation therapy or other treatments during the trial (12%), current age or health status (9%), and insufficient evidence of efficacy (7%). Notably, a response of none/nothing was given by 8% of respondents.
Discussion
This study is the first to assess knowledge, attitudes, and preferences related to gene therapy in individuals with AATD. Our results indicate a wide range of AATD gene therapy knowledge among our study population, and that, generally, knowledge is highest regarding AATD-specific etiology and genetics, moderate regarding clinical trials, and low regarding genes, gene expression, and genetic therapies. Even for AATD-specific knowledge, the average participant answered only 67% of questions correctly, highlighting gaps in understanding and areas for enhanced and continued educational initiatives. Knowledge gaps were more pronounced in other areas, yet participants were aware of gaps (the unsure response rate was more than double the incorrect response rate). Participants reported high interest in learning more about gene therapies and clinical trials and expressed support of ongoing gene therapy development. Interestingly, the most frequently endorsed desire was for general/nonspecific information, suggesting uncertainty of what types of information exist and could be helpful.
The participant characteristic most associated with higher knowledge was having attended an AATD-specific conference or educational event, reflective of the educational value of these events. Other factors associated with greater knowledge included a higher level of education, a longer time since diagnosis, having a genotype associated with high risk for lung disease, and being younger than 65. A high disease risk may intrinsically motivate individuals to learn about their condition and may contribute to more frequent or robust medical attention, serving as learning opportunities. Additionally, those who have been diagnosed longer have had more time, and likely more exposure, to acquire and internalize complex information that extends beyond general knowledge. Therefore, efforts to educate individuals with AATD on gene therapies should be highly visible and accessible, start with basics, provide continuous opportunities for reinforcement and new learning, and be re-evaluated over time.
Given the high level of trust endorsed in organizations like the Alpha-1 Foundation and AlphaNet, as well as health care providers who care for individuals with AATD, it is important that these organizations and providers are prepared to serve as a source of information and guidance on gene therapies. Findings of this study also mirror results of previous studies in other genetic conditions, including sickle cell disease, inherited retinal diseases, Friedreich ataxia, and phenylketonuria, which similarly found a relative lack of knowledge about gene therapies,16-18,25,26,29 with awareness of the knowledge deficit and desire for additional information and learning opportunities.28 Synergy between rare disease communities might also be an avenue to amplify educational efforts.22
Understanding patient attitudes and preferences regarding gene therapies is an important aspect to ensure therapies are acceptable to the population. Gene therapy trial characteristics that would increase or decrease the likelihood of participation largely corresponded with AATD clinical features and patient experiences. For example, a therapy capable of targeting both liver and lung disease is preferred over one that only targets lung disease (the most common problem in AATD), which was preferred over one that only targets liver disease. As expected, there was a clear preference for gene therapies that require the least frequent re-dosing, with highest preference for one not requiring re-dosing and decreased preference as re-dosing frequency increased. While this relationship seems logical for any population, it is particularly meaningful to the alpha-1 community given its familiarity with the burden associated with regular augmentation therapy infusions. The preferences displayed by our study population are aligned with those displayed by populations with other genetic conditions in previous studies. This demonstrates consistent preference for gene therapies (or gene therapy trials) that are efficacious in addressing the most relevant health concerns, have a good safety profile, maintain eligibility for future trial participation, minimize the burden of treatment or trial participation, do not include a chance of receiving placebo, and are well-explained and understood.16,18-21,26,27,29
Previous studies have found conflicting results regarding the relationship between knowledge related to gene therapy and attitudes and/or preferences regarding gene therapy. In some cases, increased knowledge is associated with more concerns and/or less positive attitudes towards gene therapy. In others, greater knowledge is associated with more positive attitudes about gene therapy.16-18,27 Our study examined the relationship between participant knowledge related to AATD gene therapy, attitudes towards gene therapies, and preferences regarding potential characteristics of a gene therapy for AATD. In this alpha-1 cohort, individuals with greater gene therapy knowledge reported more positive attitudes towards gene therapy and were more willing to participate in a gene therapy clinical trial or receive an approved gene therapy. Thus, the benefit of educational efforts and materials may extend beyond the individual learner and facilitate trial enrollment and therapy uptake.
While results of this study offer insights for gene therapy development, trial design, and patient education, there are several limitations. Individuals who participated represent 25% of the invited AlphaNet population and may differ from the larger AlphaNet cohort and/or the larger community of individuals with AATD. Respondents may represent a more informed and engaged subset of the alpha-1 community, which could overestimate knowledge levels and favorable attitudes toward gene therapy. Future efforts to improve response rates may include adding a subsequent follow-up or reminder, direct contacts, multimodal recruitment (e.g., phone outreach, paper surveys, or in-clinic recruitment), or additional incentives. Leveraging trusted sources such as alpha-1–specific organizations and care teams may further enhance engagement. Respondents were 98% White, non-Hispanic, similar to previous studies of the AATD population. This is reflective of the higher prevalence of AATD in White, non-Hispanic individuals and health care inequities that lead to AATD being underdiagnosed in communities with higher underrepresented minority rates.30-32 Thus, the response rate and racial/ethnic distribution of our study population may limit the generalizability of our results. Future work should focus on targeting more diverse or less-engaged populations. Another limitation is that some clinical characteristics of the study population are self-reported and thus, subject to recall bias. Additionally, while the research instrument was carefully developed by the study team and in consultation with members of the alpha-1 community to assess relevant knowledge, attitudes, and preferences related to gene therapy for AATD, it is a novel instrument that has not undergone formal validation and may have missed relevant domains related to knowledge, attitudes, and preferences in this population.
Conclusion
Participants with AATD demonstrated variable gene therapy knowledge, with many expressing awareness of their limited understanding, as well as a desire for additional information about the benefits, risks, and limitations of gene therapy, and a better understanding of the logistics of receiving gene therapy and how gene therapies work. Although perceptions of gene therapy were favorable, overall, those with higher knowledge scores were more supportive of gene therapy and more likely to participate in a gene therapy clinical trial. Thus, increasing patient access to gene therapy education may benefit trial enrollment and accelerate development. Our results support that AATD-supportive organizations and health care providers who treat patients with AATD are highly trusted and influential, and therefore, are ideally poised to provide gene therapy education and information. The responses to this study’s knowledge-based questions, along with the summary of participants’ open-ended responses, may be used to inform the development of future educational resources and guides for both patients and providers. This report of the alpha-1 community’s attitudes and preferences regarding gene therapies can contribute to the development of therapies and clinical trials that are in line with the community’s preferences and expectations. These findings support the integration of structured, clinician-delivered education and preference elicitation into shared decision-making. This will ensure patients are adequately informed and engaged when considering gene therapy options, enhance patient confidence, reduce decisional uncertainty, and improve alignment between patient values and emerging therapeutic choices.
Acknowledgements
Author contributions: MMS, KEF, GH, SNM, and CS were responsible for the conception of the study. All authors contributed to the design of the study. CS supervised the study. KEH was in charge of data collection and curation, and MMS and CS were responsible for data analysis and interpretation. MMS and KEF wrote the initial draft, and KEH wrote the IRB approval documents and recruitment and supporting documents. RAS, KEF, GH, SNM, and ML revised the research instrument, and all authors revised the manuscript. MMS and KEF wrote the revisions, and KEF was responsible for the final draft of the manuscript. All authors reviewed and approved the final version of the manuscript submitted for publication.
Declaration of Interest
KEH receives consulting income from AlphaNet. RAS reports a leadership role with AlphaNet, is on advisory committees for Beam, and has nondisclosure agreements with Wave Life Sciences, Tessera, AiRNA, and UniQue. CS reports a leadership role with AlphaNet, and has consulted for Beam, KorroBio, Takeda, and Wave Life Sciences with monies donated to AlphaNET, and has clinical trials initiated with Beam, Krystal, Takeda, and Tessera that involve genetic therapies with monies paid to the Medical University of South Carolina. KEF received past consulting income from AlphaNet. SNM receives funds for research consultation from AstraZeneca. MMS, GH, and ML have no relevant financial or nonfinancial interests to disclose.