Running Head: Bronchiectasis and Menopause
Funding Support: None
Date of Acceptance: May 27, 2026 | Published Online Date: June 3, 2026
Abbreviations: aHR=adjusted approximate hazard ratio; BMI=body mass index; CI=confidence interval; CM=Clinical Modification; HT=hormone therapy; ICD=International Classification of Diseases; IQR=interquartile range; NR=not reported; WHI=Women’s Health Initiative
Citation: Geyer AI, Sacco SJ, Shadyab AH, Metersky ML. Reproductive lifespan and adult-onset bronchiectasis in U.S. postmenopausal women: an investigation of the Women’s Health Initiative cohort. Chronic Obstr Pulm Dis. 2026; 13(4): 316-327. doi: http://doi.org/10.15326/jcopdf.2025.0740
Online Supplemental Material: Read Online Supplemental Material (311KB)
Introduction
Bronchiectasis is a condition characterized by pathologic dilatation of bronchi associated with inflammation, infection, and chronic productive cough.1-3 Recent estimates suggest approximately 400,000 people in the United States have this condition.4 Bronchiectasis is almost twice as common in women as in men, and its prevalence increases rapidly in the sixth decade of life.4,5 The median age of natural menopause in women from industrialized countries is around 50–52 years.6 Yet, whether the increased prevalence of bronchiectasis after menopause is a function of age independent of menopause, or whether menopausal transition itself increases the risk of bronchiectasis is not known.
The effects of female reproductive hormones on airway diseases and immunity are complex.7-9 On the one hand, estrogen exposure may be responsible for the increased disease severity observed in postpubertal females compared to males with cystic fibrosis by impairing mucociliary clearance or inducing phenotypic conversion of Pseudomonas aeruginosa (P aeruginosa) to a more pathogenic mucoid form in the cystic fibrosis airways. On the other hand, cessation of estrogen production at menopause is believed to contribute to immune senescence10 and may predispose to airway infection. For example, in murine models, ovariectomy-induced estrogen deprivation increases pulmonary burden of Mycobacterium avium (M avium),11 a pathogen frequently associated with (and possibly causative of) bronchiectasis, particularly in women. It is conceivable that earlier menopausal transition, by reducing the immune-stimulating effects of estrogen and increasing the risk of airway infection, contributes to the risk of bronchiectasis development in women. Yang et al attempted to address this possibility in a population-based study of >1,000,000 Korean women. They found that shorter duration of reproductive lifespan (menarche to menopause) was a risk factor for bronchiectasis in postmenopausal Korean women.12
No comparable study has been performed in the United States. Yet significant differences in reproductive factors exist between the 2 populations. For example, early menopause is twice as common in Korean women, while early menarche is twice as common in U.S. women.13 To address a gap in knowledge about population-specific association between reproductive factors and the risk of bronchiectasis in postmenopausal women, we performed analysis of a prospective cohort of U.S. female participants of the Women’s Health Initiative (WHI).
The WHI is a long-term national health study14 of 161,808 postmenopausal women aged 50 to 79 years old recruited from 40 clinical centers across the United States between 1993 and 1998. The study cohort included 93,676 women in the observational arm and 68,132 in the interventional arm (overlapping trial participation): hormone therapy (HT) (N=27,347), calcium and vitamin D supplementation (N=36,282), and diet modification (N=48,835). WHI enrolled a wide range of postmenopausal women with a racial and ethnic make-up similar to the U.S. population of the same age range at that time.15 Medicare claims data were linked to a large fraction of the study participants. The purpose of this study was to determine the association between reproductive factors (i.e., duration of the reproductive lifespan and age at menopause) and incidence of bronchiectasis in a sample of U.S. postmenopausal women enrolled in the WHI.
Methods
Ethics Statement
The study was approved by the UConn Health Internal Review Board.
Dataset and Cohort
We examined baseline data from the WHI study to obtain participant demographics, reproductive characteristics, and lifestyle habits. We examined Medicare claims data linked to these participants, extracting International Classification of Diseases (ICD) versions 9 and 10 diagnosis codes of bronchiectasis, known causes of bronchiectasis, and related comorbidities.
In Figure 1, we summarize the results of our cohort selection procedure. A total of 161,808 postmenopausal women were enrolled in WHI. Of these, 145,995 had Medicare claims data available (enrollment dates between 1991 and 2022). To capture all diagnostic encounters, we only included participants with fee-for-service Medicare A or B coverage (N=127,871). To avoid missing diagnoses due to lack of coverage, we excluded participants with any coverage gap ≥1 year (N=21,322). In addition, we excluded participants <65 years old at Medicare enrollment (N=4685) since early enrollment would indicate the presence of significant physical or mental disability, end stage renal disease, or amyotrophic lateral sclerosis, and potentially distort our findings. Lastly, we excluded participants with missing reproductive history data at baseline (N=6179). The resulting cohort of 96,996 women was followed from Medicare enrollment to the first incidence of bronchiectasis, death, loss to follow-up, disenrollment from fee-for-service Medicare, or administrative end of follow-up (December 31st, 2022), whichever came first.
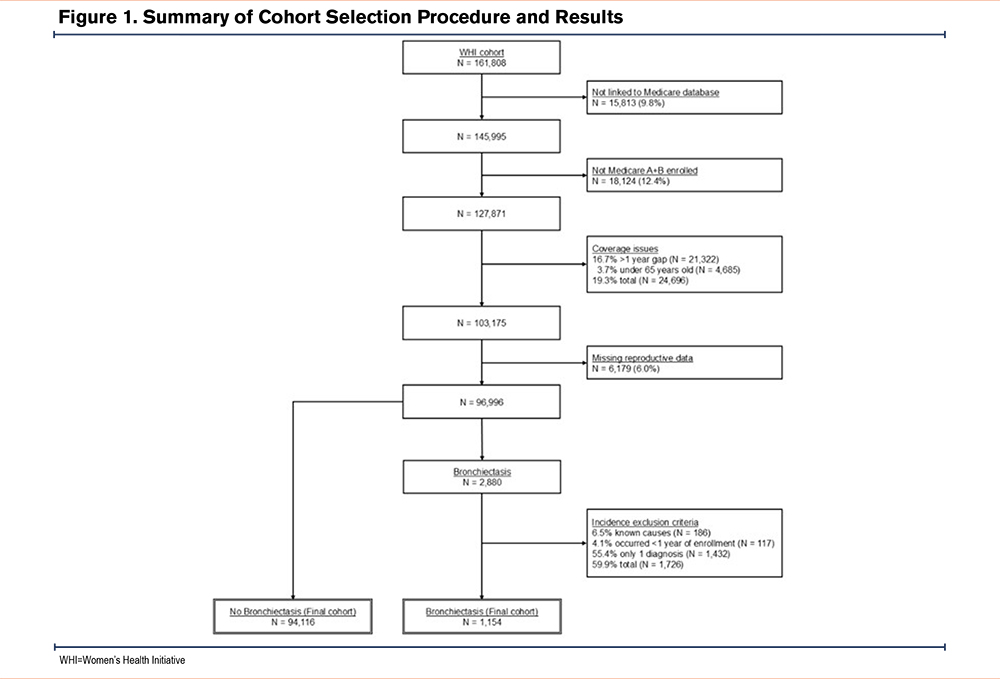
The first incidence of bronchiectasis diagnosis documented in participants’ records as either ICD-9 494.XX or ICD-10 J47.XX was recorded as their index event, resulting in 2880 cases. Given our focus on adult onset bronchiectasis, we excluded 186 participants with prior or concurrent diagnoses of cystic fibrosis (ICD-9: 748.61, 277; ICD-10: Q33.4, E84), primary ciliary dyskinesia (ICD-9: 759.3; ICD-10: Q34.8, Q89.3), Mounier-Kuhn syndrome (ICD-10: Q32.4), allergic bronchopulmonary aspergillosis (ICD-10: B44.81), or relevant immunodeficiency syndromes (ICD-9:042, 279.0–279.53; ICD-10: D80–84, B20). Further, to capture only newly occurring bronchiectasis diagnoses (and not the pre-existing diagnoses), we excluded 117 bronchiectasis participants who had diagnoses within one year of Medicare enrollment. Our final cohort included 2586 women with incident bronchiectasis and 94,116 without this condition.
Study Variables
Demographics included self-reported age at WHI baseline, race (coded as Black or African American, White, and other or multiple races), ethnicity, income status, education level, and body mass index (BMI) (weight in kg/height in 2). We also included the age at Medicare enrollment for use in time-to-event analyses.
Reproductive characteristics included self-reported age at menarche and age at menopause as determined by the WHI algorithm16 considering last menstrual bleeding, bilaterial oophorectomy, age at HT, and overall age. We calculated reproductive lifespan as the difference between the ages at menopause and menarche. We coded age at menarche as <12 and ≥12 years old, and age at menopause as <40, 40–44, 45–49, 50–54, and ≥55 years old.17 We coded reproductive lifespan as <30, 30–34, 35–39, ≥40 years old.12 Additionally, we defined surgical menopause as bilateral oophorectomy prior to, or at, age at menopause. We defined HT as any self-reported use at or within the 10 years before WHI enrollment, or being enrolled in one of the HT arms of the WHI trial (i.e., estrogen or estrogen+progesterone arms). We also assessed self-reported use of any oral contraceptives, and parity (no children, one child, multiple children).
Lifestyle habits included moderate or rigorous recreational physical activity (minutes/week), alcohol use (drinks/week), and smoking behavior (never, former, or current use).
Comorbidities related to bronchiectasis were obtained from Medicare claims (if bronchiectasis occurred, we only recorded comorbidities that preceded the bronchiectasis diagnosis). Specific conditions and their corresponding ICD-9 and -10 codes are provided in the supplemental materials (e-Appendix 1 in the online supplement).
Statistical Analysis
We described study variables using frequencies and proportions for categorical variables and medians and interquartile ranges (IQRs) for continuous variables. To compare study variables by reproductive lifespan and bronchiectasis occurrence, we utilized Chi-squared tests, Kruskal-Wallis tests, and Wilcoxon ranked sum tests where appropriate. To account for multiple comparisons, we adjusted p-values using Bonferroni correction. Note, for multiple comparisons of variables with more than 2 groups, we compared single groups (e.g., White race) to all other groups (e.g., Black or African American and other races pooled together).
To describe the time between Medicare enrollment and first bronchiectasis diagnosis (i.e., time-to-event), we calculated incidence rates per 1000 person-years by categorical study variables. To compare time-to-event by reproductive lifespan categories, age at menarche and menopause categories, we created 3 Cox proportional hazards models. All models controlled for age at Medicare enrollment, race, ethnicity, BMI, smoking behavior, surgical menopause, HT use, oral contraceptive use, parity, and comorbid conditions. For each model, we tested the proportional hazards assumption using Grambsch-Therneau tests18 and log-minus-log plots. We explicitly described and handled any violations dependent on their severity and characteristics. For women who did not have an event, we censored their data at the end of their last Medicare enrollment period or death if it occurred. We estimated linear and nonlinear trends in bronchiectasis incidence over reproductive characteristic values by creating 3 additional models, identical to the 3 above, but utilizing the continuous reproductive variables rather than the categorical ones. To remain cautious of possible multicollinearity between reproductive characteristics and control variables, we calculated variance inflation factors for continuous reproductive characteristics as predicted by control variables. We considered values <2 to indicate little to no multicollinearity. As HT use was theorized to modify the hypothetical relationship between reproductive factors and bronchiectasis, we conducted the analyses above again including an interaction term between the assessed reproductive characteristic and HT use. For any models with linear or nonlinear trends between reproductive characteristics and bronchiectasis risk that statistically differed by HT use, we calculated trends and categorical differences by HT use via simple slopes analysis.
Since the rates of missingness were minimal in our study (most <1%; one variable, physical activity was 3%), we utilized median replacement. All analyses were conducted in R19 version 4.4.1. Alpha for 2-sided tests was set to 0.05.
Results
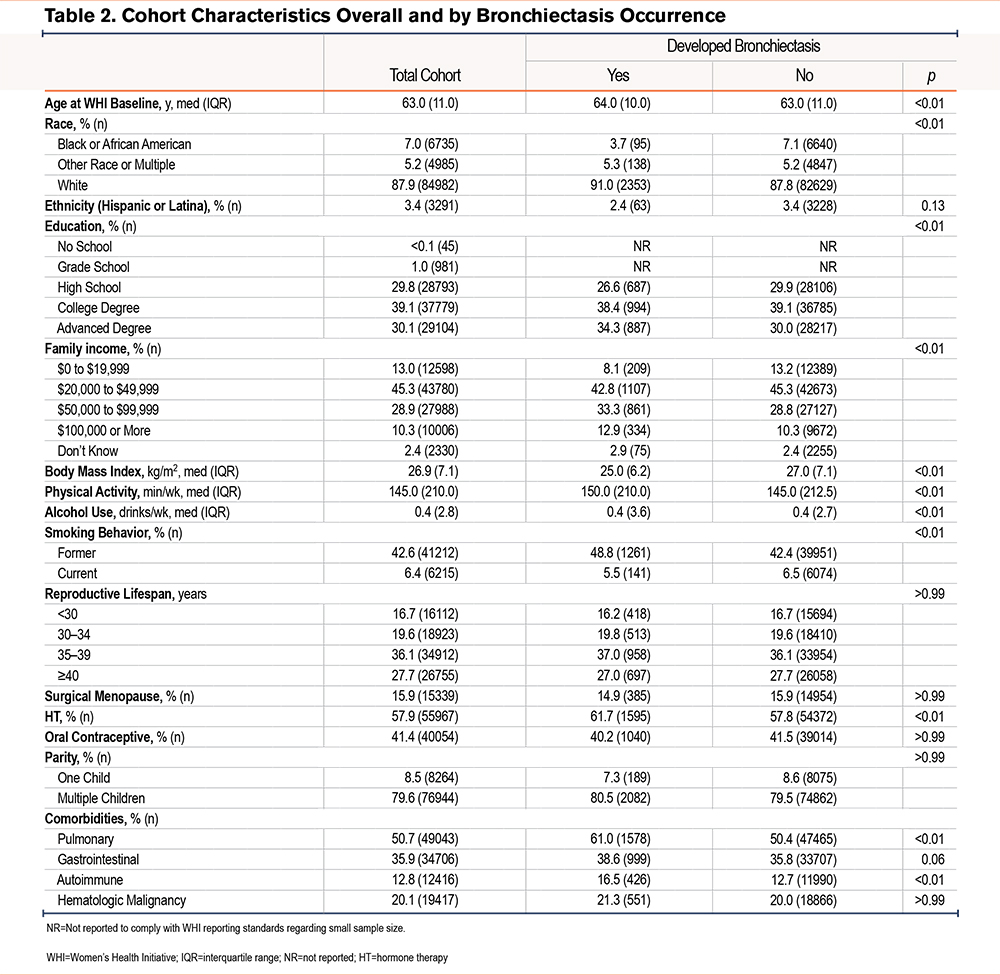
In Tables 1 and 2, we summarize cohort characteristics at WHI baseline overall and as stratified by reproductive lifespan categories and bronchiectasis occurrence, respectively. Participants were 87.9% White and 7.0% Black, while 5.2% reported another race or multiple races. A total of 3.4% of participants identified as Hispanic ethnicity. The median participant age was 63.0 years old (IQR=11.0) at WHI baseline and 65.0 years old (IQR=2.3) at Medicare enrollment. Almost half of the cohort were former tobacco smokers (42.6%), while far fewer were current smokers (6.4%). Participants had a median reproductive lifespan of 37.0 years (IQR=8.0), median age at menarche of 13.0 years (IQR=1.0), and median age at menopause of 50.0 years (IQR=7.0). Over half of participants used postmenopausal HT (57.9%), less than half used oral contraceptives (41.4%), and around 1-in-6 (15.9%) had a bilateral oophorectomy (i.e., surgical menopause). A total of 2586 women (2.7%) had a bronchiectasis diagnosis during a median of 16 years (IQR=14) of follow-up time. Given most p-values of comparisons by reproductive lifespan and bronchiectasis occurrence were statistically significant (i.e., p<0.05), we highlight substantial differences. All reported differences below had p’s<0.01.
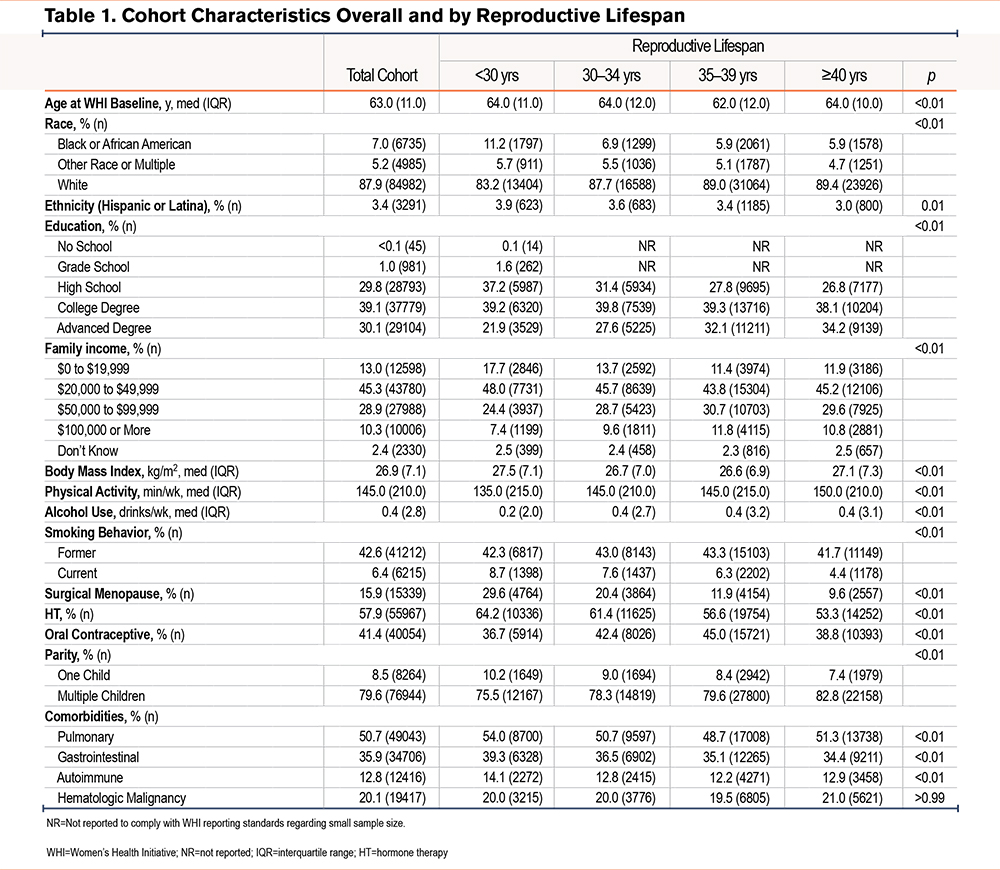
Compared to women with longer reproductive lifespans (e.g., ≥40 years), those with the shortest reproductive lifespans (i.e., <30 years) were more likely to use HT (64.2% versus 53.3%) and to have an oophorectomy (29.6% versus 9.6%).
Women with a bronchiectasis diagnosis were less likely to be Black (3.7% versus 7.1% without), had lower BMIs (25.0kg/2 versus 27.0kg/2 without), and higher rates of pulmonary conditions (61.0% versus 50.4% without). They were also more likely to use HT (61.7% versus 57.8% without). Neither surgical menopause nor oral contraceptives were associated with an increased risk of bronchiectasis development.
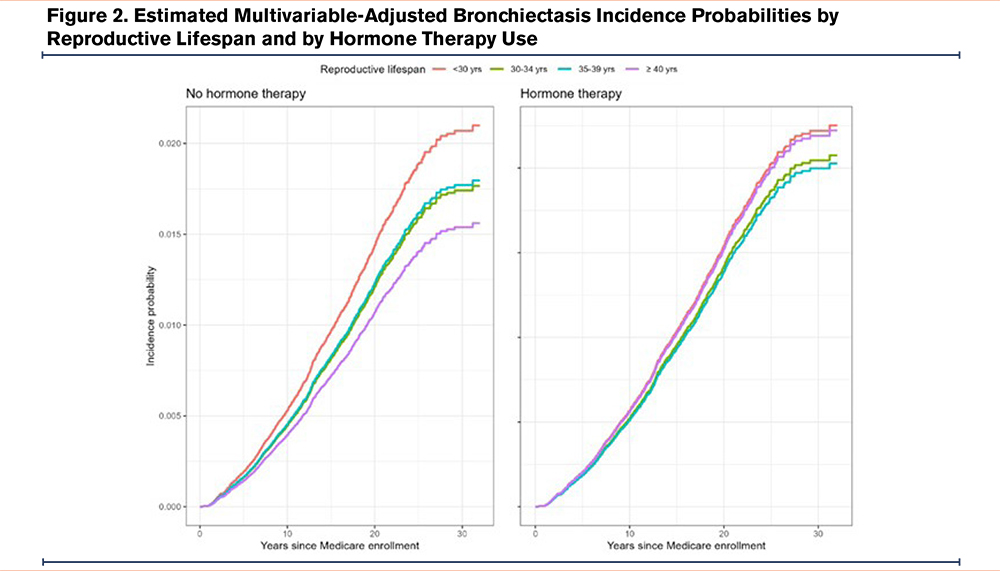
In Table 3, we present multivariable-adjusted bronchiectasis risk by reproductive characteristics overall and as modified by HT use (See e-Appendix 2 in the online supplement for adjusted bronchiectasis incidence rates). A shorter reproductive lifespan was associated with higher bronchiectasis risk (trend p=0.01). Women with the longest reproductive lifespans (≥40 years) were at 12% lower risk of bronchiectasis than those with the shortest reproductive lifespans (<30 years; adjusted approximate hazard ratio [aHR]=0.88 [95% confidence interval (CI): 0.77, 0.99]). HT use modified this relationship (interaction p=0.04), such that a shorter reproductive lifespan was associated with bronchiectasis risk in women without HT use (trend p=0.01), but not in women who used HT (trend p=0.23). Specifically, among women with no HT, the longest reproductive lifespans were associated with a 22% lower risk of bronchiectasis compared with the shortest reproductive lifespans (aHR=0.78 [95% CI: 0.62, 0.94]) (Figure 2).
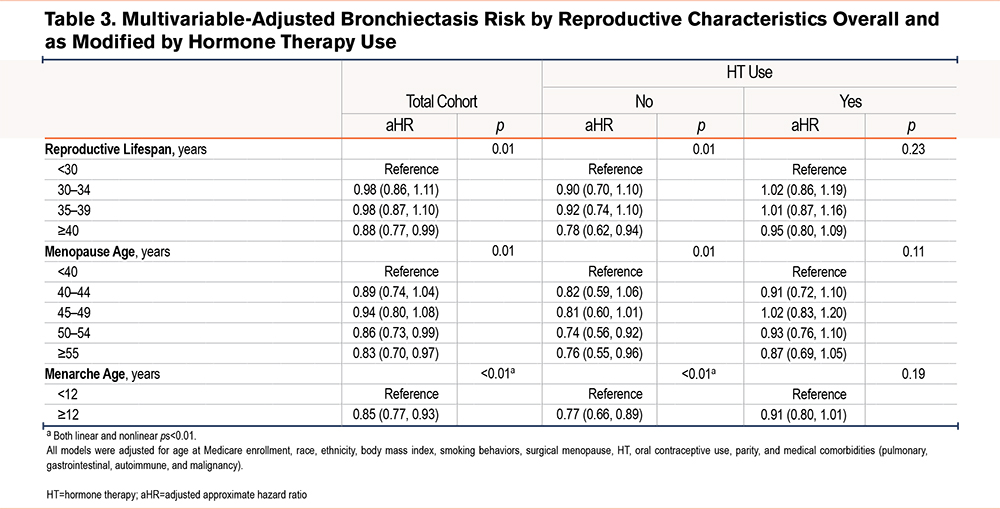
Comparable results were found for menopause age. The age of menopause was related to risk of bronchiectasis (trend p=0.01), whereby women with later ages of menopause were at 14% (50–54 years) and 17% (≥55 years) lower risk of bronchiectasis than those with the earliest ages (<40 years) (aHRs=0.86 [95% CI: 0.73, 0.99] and 0.83 [95% CI: 0.70, 0.97], respectively). HT use did not statistically significantly modify this relationship (interaction p=0.10); however, age of menopause was related to a risk of bronchiectasis only among the women who did not use HT (trend p=0.01) and not among those who used HT (trend p=0.11). Among non-HT users, women with later ages of menopause (50–54 and ≥55 years) were at lower risk than women with an early age of menopause (<40 years; aHRs=0.74 [95% CI: 0.56, 0.92], and 0.76 [95% CI: 0.55, 0.96], respectively). Lastly, an earlier age of menarche was related to a higher risk of bronchiectasis (trend p<0.01), whereby women with later ages of menarche (≥12 years) were at 15% lower risk than women with earlier ages of menarche (<12 years; aHR=0.85 [95% CI: 0.77, 0.93]). HT use modified this relationship (interaction p<0.01), such that the age of menarche was associated with bronchiectasis risk among the women who did not use HT (trend p<0.01) but not in those who used HT (trend p=0.19). Specifically, among women who did not use HT, those with later ages of menarche (≥12 years) were at lower risk than women with an earlier age of menarche (<12 years; aHRs=0.77 [95% CI: 0.66, 0.89]).
Across all models, women who used HT were at 19% greater risk of bronchiectasis (p’s<0.01; e.g., reproductive lifespan trend model aHR=1.19 [95% CI: 1.08, 1.27]).
Posthoc Analysis
While we defined bronchiectasis cases by the presence of at least one mention of the corresponding ICD-9/10 code to increase our sensitivity, some diagnoses may have been recorded only for the purpose of further testing, leading to a decreased specificity. Subsequently, we re-ran the above analyses requiring 2 occurrences of the bronchiectasis ICD code for case definition (e-Appendix 3 in the online supplement). This cohort contained 95,270 women with 1154 bronchiectasis cases (1.2%). The associations described above generally persisted, although weakened. The primary difference was that the relationship between reproductive lifespan and bronchiectasis risk did not reach statistical significance in the overall cohort (trend p=0.07), and reproductive group differences were less consistent.
Discussion
We studied a cohort of >100,000 postmenopausal women with a median follow-up of 16 years enrolled in the WHI and fee-for-service Medicare and found that, among women without HT use, the risk of incident bronchiectasis decreased with longer reproductive lifespans. A reproductive lifespan was defined as the difference between the ages of menopause and menarche. The observed effect of the reproductive lifespan was driven primarily by the age of menopause onset which ranged widely from <40 to >55 years. The risk of bronchiectasis decreased as the menopause age increased. The range of age of menarche was much narrower and, while earlier menarche age appeared to increase the risk of bronchiectasis, the cumulative effect was heavily influenced by the age of menopause. Our findings are consistent with those of Yang et al12 who identified shorter reproductive lifespan as a risk factor for bronchiectasis in a population of Korean women.
One plausible explanation for this finding is that low postmenopausal estrogen levels predispose women to respiratory tract infections by several pathogens, including M avium, which has been closely associated with bronchiectasis in women.20 Indeed, women with M avium lung disease have been found to have lower circulating levels of estradiol than healthy controls.21 Furthermore, ovariectomized mice infected with M. avium demonstrated higher pulmonary organism burden than sham-operated controls, and exogenous estrogen replacement eliminated this difference.11
We also found that HT use modified the effect of association between reproductive lifespan and the risk of bronchiectasis in the full cohort and appeared to nullify this relation within women with HT use completely. Furthermore, HT use was associated with greater risk of bronchiectasis regardless of reproductive span duration or age at menopause, suggesting that HT use may itself be a risk factor. This finding is also consistent with Yang’s study of Korean women in which HT for ≥5 years was associated with a higher risk of bronchiectasis.12 The finding that longer reproductive lifespan (and the correspondingly longer exposure to estrogen) is associated with a reduced risk of bronchiectasis while estrogen replacement is associated with an increased risk appears paradoxical. One likely explanation for this paradox is the possibility of reverse causality, such that the women who had the greatest postmenopausal estrogen deficiency (and were most predisposed to bronchiectasis) were also more likely to receive postmenopausal HT.
Alternatively, estrogen may not in fact be protective. In people with cystic fibrosis, the risk of exacerbations and disease severity are greater in postpubertal females versus age-matched males (while the opposite is true prior to puberty).22 This may in part be due to the negative effects of estrogen on mucociliary clearance and the increased virulence of P aeruginosa promoted by estrogen.23 If estrogen itself is not protective, and even harmful, in this context, perhaps it is not the duration of reproductive hormone (including estrogen) exposure itself that reduces the risk of bronchiectasis. Rather, an upstream genetic, epigenetic, or environmental process may be responsible for both—the longer reproductive lifespan and the lower risk of bronchiectasis. Of note, later onset of menopause is known to be associated with greater longevity. While some of the benefits are mediated by estrogen, there is evidence for shared genetic determinants of both independent of estrogen exposure. For example, several DNA-damage response and immune function genes have been associated with age at menopause.24 It is conceivable (though admittedly a mere speculation) that some of the biologic pathways that delay ovarian aging and menopause,25 may serve to delay or prevent bronchiectasis independent of estrogen exposure.
Our study has important strengths including a large study sample (>100,000 women), and a relatively long duration (median of 16 years). Study participants had exceptionally detailed characterization of demographic and lifestyle factors and the rate of data missingness was very low (<3%). We also were able to take advantage of rich Medicare claims data with information on bronchiectasis and comorbidities.
There are several limitations to our study. The diagnosis of bronchiectasis was obtained from Medicare claims data using ICD-9 Clinical Modification (CM) and ICD-10-CM codes and could not be independently verified. ICD codes are primarily used for billing purposes and only secondarily for epidemiologic research.26 The use of ICD codes for identifying cases of bronchiectasis is not formally validated in the U.S. Medicare population, but has been used by previous investigators.4,5 We used the same case definition as Seitz et al5 i.e., presence of at least one ICD-9/10 code in Medicare claims data. This increased the likelihood of detecting most cases, including mild ones, but may have also resulted in including “suspected” diagnoses.4,5 Thus, our case definition may have provided the “upper bound” of bronchiectasis incidence. Due to this fact, we performed a sensitivity analysis requiring 2 bronchiectasis diagnoses, which dropped incidence from 2.7% to 1.2%. Despite this, associations between reproductive characteristics and bronchiectasis onset remained mostly unchanged, minimizing our concerns regarding this decision.
Accuracy of diagnostic coding in general27 and for bronchiectasis specifically28 has been questioned. For instance, Green et al28 found that ICD-9/10 codes identified only 34% of radiologically-diagnosed bronchiectasis. It should be noted, however, that the currently accepted case definition of bronchiectasis includes both symptoms (e.g., cough, mucus production, exacerbations) and radiographic confirmation of dilated airways.29 In Green’s study, however, most of computed tomography-identified bronchiectasis was incidental. When patients’ charts and imaging were independently reviewed by 3 separate observers, only 29% met the consensus case definition criteria. This suggests that, while ICD codes might underdiagnose bronchiectasis, the true sensitivity of ICD codes is likely higher than 34%.
While, as discussed above, our case definition may be prone to both under- and over-diagnosis, it is unlikely that the frequency of ICD-9/10 codes was differentially distributed among the reproductive span or menopause age quantiles and, therefore, is unlikely to have biased our results. Additionally, without employing insurance claims data, it may be impossible to leverage the existing large-scale, informative databases, such as the one used in our study, to answer important research questions. Our work and others should be considered in the scope of this limitation, as it will likely remain a standing limitation of this type of research.
The absence of diagnostic data prior to Medicare enrollment did not allow us to study bronchiectasis diagnosed earlier than age 65. It should also be noted that diagnosis of bronchiectasis and incidence of disease are not the same and that bronchiectasis was likely developing for a number of years prior to the diagnosis. To minimize the risk of mistaking prevalent cases of bronchiectasis at the time of Medicare enrollment for incident bronchiectasis, we excluded the cases documented for the first time during the first year on Medicare (i.e., prior to age 66) from analysis of incidence. This might have resulted in underestimating the total number of cases in our cohort. Surprisingly, only 4.1% of all cases of bronchiectasis were reported during the first year of Medicare enrollment. This might reflect a truly low prevalence rate of this condition in women younger than 66 years of age or underdiagnosis. Alternatively, pre-Medicare-enrollment cases may not have been recorded until later, which would result in underestimating disease prevalence at the age of 66 and overestimating its incidence after 66. In addition, exclusion of women with >1 year gap in fee-for-service Medicare coverage (~17% of total) may have introduced selection bias. It is unknown whether Medicare recipients on fee-for-service Medicare are different from those in Medicare Advantage programs. It seems unlikely, however, that there would be a significant difference between the 2 in terms of reproductive span or menopause age. Regarding lack of documentation of pre-existing comorbidities and possible causes of bronchiectasis prior to Medicare enrollment, there is no known solution when utilizing this data source, and this remains a limitation of this study and other studies alike.
Lastly, many women in our cohort had diagnoses of pulmonary conditions and reported either former or current smoking behaviors. While we controlled for both of these factors in our models (helping isolate the unique association between reproductive characteristics and bronchiectasis), it is still possible that our findings may not generalize well to populations with lower rates of pulmonary conditions and smoking behaviors.
In summary, our study demonstrated that longer reproductive life span duration (or later menopause age) was associated with a lower risk of bronchiectasis diagnosis in women after the age of 66, especially without HT use. To our knowledge, this is the first such study in the United States. Additional studies are needed to answer such questions as: (1) whether there is a genetic or environmental predisposition to both a shorter reproductive lifespan and bronchiectasis25; (2) by what mechanisms might estrogen, progesterone, or other ovarian hormones affect airway biology relevant to bronchiectasis, such as effects on mucociliary clearance or immune response to infection; and (3) whether the use, type, and/or duration of HT might reduce or exacerbate the risk and severity of bronchiectasis in postmenopausal women.
Acknowledgements
Author contributions: AIG conceptualized the manuscript. AIG, SJS, AHA, and MLM designed the work. SJS was responsible for the acquisition and analysis of the data, and AIG, SJS, AHA, and MLM interpreted the data. SJS drafted the methods portion of the manuscript. AIG, AHA, and MLM drafted the manuscript. All authors edited the manuscript. AIG, SJS, AHA, and MLM gave final approval of the manuscript. AIG is accountable for the accuracy and integrity of the manuscript.
Other acknowledgements: The authors would like to acknowledge the WHI investigators:
Program Office: (National Heart, Lung, and Blood Institute, Bethesda, Maryland) Jacques Rossouw, Jared Reis, and Candice Price Clinical Coordinating Center: (Fred Hutchinson Cancer Center, Seattle, WA) Garnet Anderson, Ross Prentice, Andrea LaCroix, and Charles Kooperberg
Steering Committee and Academic Centers: (University of Alabama at Birmingham) Gretchen Wells; (Albert Einstein College of Medicine) Yasmin Mossavar-Rahmani; (University at Buffalo) Amy Millen; (University at Buffalo) Jean Wactawski-Wende; (Fred Hutchinson Cancer Center) Marian Neuhouser; (Fred Hutchinson Cancer Center) Holly Harris; (University of Massachusetts) Brian Silver; (University of North Carolina) Nora Franceschini; (Stanford Prevention Research Center) Marcia L. Stefanick; (The Ohio State University) Electra Paskett; (Wake Forest University) Mara Vitolins.
Declaration of Interest
MLM has received consulting fees from Boehringer Ingelheim, Insmed Incorporated, Tactile Inc., and Zambon; served on data safety monitoring boards for AN2 Therapeutics, Renovion, and Verona; and received clinical trial support to the University of Connecticut from Insmed, Armata, and Sanofi. AG, SS, and AS have nothing to declare.